


Prolonged Fever of Unknown Origin With Suspicion of Adult-Onset Still’s Disease: A Diagnostic Challenge
DOI:
https://doi.org/10.14740/jmc5291Keywords:
Fever of unknown origin, Still’s disease, Adult-onset, Rheumatology, FeversAbstract
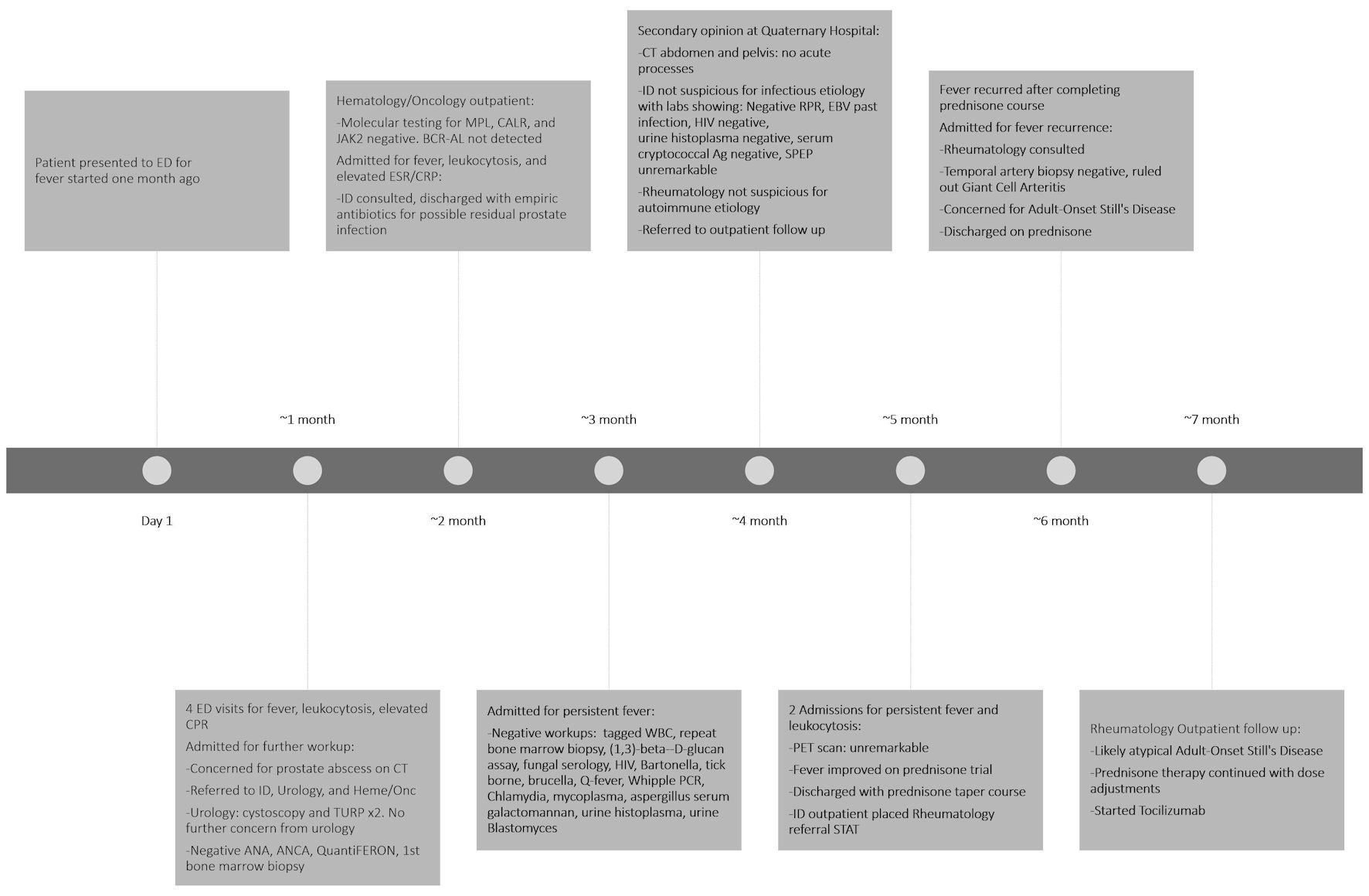
We report a 72-year-old patient with intermittent fever for 7 months, accompanied by leukocytosis, tachycardia, myalgias and arthralgias. Prior evaluations—including imaging, cultures, bone marrow biopsy, serologies, and autoimmune panels—were unrevealing. The patient’s persistent fever was previously diagnosed as fever of unknown origin (FUO), which is defined by a core temperature exceeding 38.0 °C for more than 3 weeks with no defined causes during ≥ 3 inpatient days or ≥ 3 outpatient visits. The patient’s fever initially improved with steroids. During the hospital course, empiric antibiotics were started and discontinued following negative blood cultures, and prednisone was reinitiated at discharge. There was high suspicion for atypical adult-onset Still’s disease (AOSD), and the patient was treated in the outpatient setting with steroids and tocilizumab. This case highlights the importance of systematic evaluation, multidisciplinary collaboration, and careful selection of pharmacological therapy and invasive procedures in the workup of FUO, especially in an elderly patient. The case also illustrates the challenges in diagnosing AOSD due to the highly variable clinical presentation and low prevalence, and further outlines current treatment recommendations for AOSD, which include corticosteroid therapy in combination with an interleukin (IL)-6 inhibitor.
Published
Issue
Section
License
Copyright (c) 2026 The authors

This work is licensed under a Creative Commons Attribution 4.0 International License.






