


Management of Multilevel Mid-Cervical Fractures in an Adult With Osteopetrosis
DOI:
https://doi.org/10.14740/jmc5205Keywords:
Osteopetrosis, Cervical spine fracture, Conservative management, Rigid cervical collar, Computed tomographyAbstract
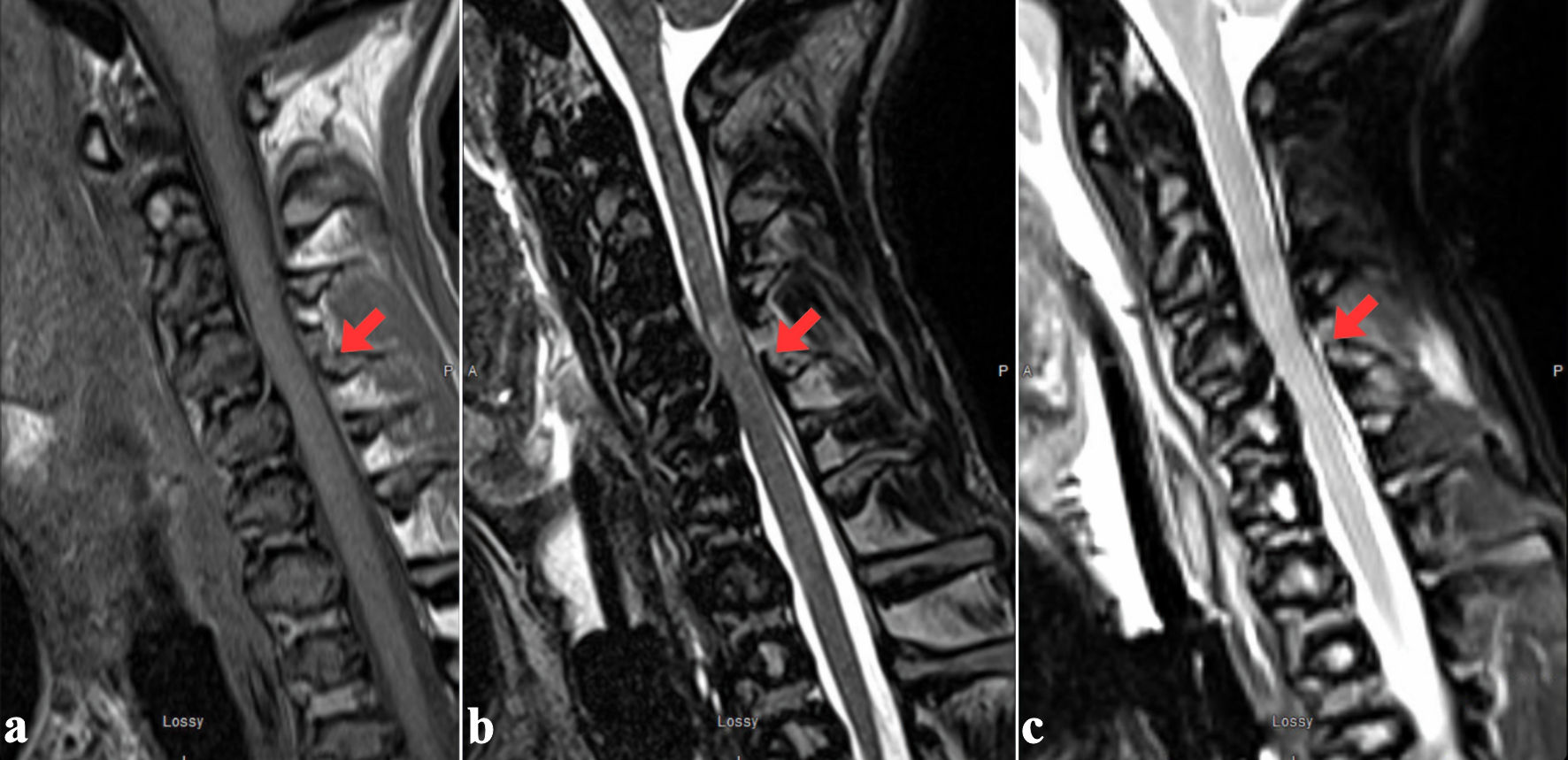
Osteopetrosis is a rare inherited osteoclast dysfunction disorder that produces bone that is both abnormally dense and brittle, complicating fracture management and internal fixation. Most cervical spine injuries reported in osteopetrosis involve the craniovertebral junction (C1-C2) and are treated surgically because of presumed instability. Reports of multilevel mid-cervical fractures with ligamentous injury successfully treated nonoperatively are exceedingly scarce. We present the case of a 22-year-old man with longstanding osteopetrosis who sustained high-energy trauma resulting in a displaced posterior-inferior C4 body fracture with associated left C4 lateral-mass involvement, nondisplaced left C3 inferior-facet and C6 pedicle fractures, and magnetic resonance imaging (MRI) evidence of focal cord T2 signal, posterior longitudinal ligament injury, and a small epidural hematoma. Despite this constellation - which, in normal bone, would often mandate operative stabilization - the patient remained neurologically intact, with acceptable alignment and negative vascular imaging. Given the unique surgical hazards of osteopetrotic bone (poor screw purchase, intraoperative fracture risk, delayed union), conservative management was chosen using a rigid cervical orthosis (Miami J®, Ossur ehf., Reykjavik, Iceland) and serial imaging follow-up. At 1 year, flexion-extension computed tomography demonstrated complete osseous bridging of the C3 facet and C4 body fractures, partial but stable bridging across the C4 facet and lamina and preserved alignment. The patient remained asymptomatic and neurologically intact. This case expands the evidence base for nonoperative management of cervical fractures in adult osteopetrosis beyond C1-C2 patterns. It highlights that rigid-collar immobilization, when neurological function and alignment are preserved and vascular injury is excluded, can yield stable union without surgery. Flexion-extension computed tomography provides a practical endpoint, supporting acceptance of stable partial radiographic healing when dynamic stability is maintained.
Published
Issue
Section
License
Copyright (c) 2025 The authors

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.






