| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://jmc.elmerpub.com |
Case Report
Volume 17, Number 7, July 2026, pages 309-320

Supportive Management of Severe Acetaminophen and Ibuprofen Overdose Twenty-Four Hours After Ingestion in Limited Resources Settings
Alert Drishtia, Entela Shkodranib, Rudin Domic, g, Ergita Nelajd, Gentian Hutie, Asead Abdylie, Filadelfo Coniglionee, Krenar Lilajc, Majlinda Nacoc, Alma Canic, Vedat Eljezif
aDepartment of Surgery, Service of Clinic Toxicology, University of Medicine, Tirana, Albania
bDepartment of Infectious Diseases, Service of Dermatology, University of Medicine, Tirana, Albania
cDepartment of Surgery, Service of Anesthesia and Intensive Care, University of Medicine, Tirana, Albania
dDepartment of Internal Medicine, Service of Internal Medicine, University of Medicine, Tirana, Albania
eDepartment of Anesthesiology and Intensive Care Medicine, American Hospital 3, Tirana, Albania
fDepartment of Perioperative Medicine, CHU Gabriel-Montpied, Clermont-Ferrand, France
gCorresponding Author: Rudin Domi, Department of Surgery, Service of Anesthesia and Intensive Care, University of Medicine, Tirana, Albania
Manuscript submitted March 30, 2026, accepted May 22, 2026, published online June 3, 2026
Short title: Late Acetaminophen and Ibuprofen Overdose Management
doi: https://doi.org/10.14740/jmc5330
| Abstract | ▴Top |
Acetaminophen and ibuprofen are among the most used analgesic–antipyretic agents worldwide, yet their combined overdose can become life-threatening, particularly when medical care is delayed. We report the case of a 29-year-old woman who presented to the emergency department more than 48 h after ingesting a massive dual overdose of acetaminophen (25 g) and ibuprofen (20 g). At admission, she complained of nausea, epigastric pain, tinnitus, and mild jaundice. Laboratory findings indicated severe acute liver injury, with markedly elevated transaminases, hyperbilirubinemia, significant coagulopathy, and metabolic acidosis, consistent with advanced acetaminophen toxicity. Due to the delayed presentation, the Rumack–Matthew nomogram was no longer reliable for risk assessment. Although antidotal therapy was indicated, neither N-acetylcysteine nor alternative antidotes were available, and options such as hemodialysis or liver transplantation were inaccessible. Management therefore relied entirely on intensive supportive care, including correction of metabolic disturbances, coagulopathy, and evolving organ dysfunction, alongside close clinical and biochemical monitoring. Despite the severity of hepatic failure and metabolic derangement at presentation, the patient showed gradual improvement over a prolonged hospital course. After 53 days of supportive therapy, liver function recovered sufficiently, and transplantation was not required according to King’s College criteria. This case illustrates that even in severe, late-presenting combined analgesic overdose complicated by acute liver failure and metabolic acidosis, a favorable outcome may still be achieved with comprehensive supportive care alone when advanced therapies are unavailable. It underscores the pivotal role of meticulous supportive management in toxicological emergencies.
Keywords: Toxicology; Overdose; Acetaminophen; Ibuprofen; Supportive treatment; Intensive care unit
| Introduction | ▴Top |
Acetaminophen and ibuprofen are among the most widely used analgesic–antipyretic agents globally. While their combined ingestion does not appear to enhance the intrinsic toxicity of either drug, overdose significantly increases the risk of serious systemic complications, as demonstrated in our case. Paracetamol poisoning remains one of the most frequent causes of drug overdose worldwide, accounting for approximately 6% of all poisoning cases and up to 56% of severe acute liver injury and acute liver failure in reported regions [1]. Despite its high incidence, outcomes are generally favorable when treatment is initiated early, with an estimated case fatality rate of 0.4% under modern management, largely attributable to the effectiveness of N-acetylcysteine (NAC) [2]. However, delayed presentation such as in our patient, substantially increases the likelihood of severe hepatotoxicity, progression to acute liver failure, and death. Within this context, our case emphasizes the importance of timely and optimized supportive therapy, especially in resource-limited settings where advanced liver support systems such as molecular adsorbent recirculating system (MARS) and specific antidotes (e.g., methionine or fomepizole) may not be available. Under these constraints, meticulous intensive care, encompassing hemodynamic stabilization, correction of metabolic disturbances, renal support, and prevention of complications, become the cornerstone of management and may be lifesaving. Thus, although overall mortality remains relatively low, the high prevalence of exposure and its role as a leading cause of acute liver failure make paracetamol toxicity a major public health concern. In our setting, at the Clinical Toxicology Service of the “Mother Teresa” University Hospital Center, combined intoxications are frequently encountered and represent true medical emergencies. Delayed hospital presentation, as seen in this case, further worsens outcomes and limits available therapeutic options.
| Case Report | ▴Top |
Investigations
A 29-year-old non-pregnant woman was admitted to the emergency department with nausea, abdominal pain, and fever. She had no relevant past medical history, was using oral contraceptives, and denied recreational drug use. On admission, vital signs were within normal limits. Physical examination revealed mild scleral icterus. In the absence of an initial toxicological history, standard supportive management was initiated while diagnostic laboratory investigations were underway.
Diagnosis
The occurrence of tinnitus and jaundice, together with laboratory findings of total bilirubin 3.04 mg/dL (normal range < 1.2 mg/dL), alanine aminotransferase (ALT) 726 U/L (normal range < 35 U/L), aspartate aminotransferase (AST) 728 U/L (normal range < 43 U/L), prothrombin time (PT) 23%, international normalized ratio (INR) 3.29 (normal range 0.8–1.2), arterial pH 7.333, partial pressure of carbon dioxide (PaCO2) 34.5 mm Hg, bicarbonate (HCO3−) 17.9 mm Hg, and base excess −7.0 mmol/L, raised strong suspicion of acute drug-induced liver injury (DILI) secondary to acetaminophen and non-steroidal anti-inflammatory drug (NSAID) overdose. This was confirmed 1 h and 25 min after emergency department admission, when the patient disclosed a deliberate suicidal self-poisoning with 25 g of immediate-release acetaminophen and 20 g of ibuprofen, reportedly occurring more than 48 h before hospital admission. The timing was based on the patient’s report and could not be precisely established; however, the laboratory findings were consistent with an ingestion occurring approximately more than 48 h before presentation.
Treatment
The presence of jaundice together with markedly elevated serum transaminases indicated progression to the hepatotoxic phase (phase II–III, > 24 h post-ingestion) of acetaminophen-induced acute liver injury, with evolving acute liver failure and its systemic consequences. At this stage, the Rumack–Matthew nomogram is no longer reliable for risk stratification; however, current toxicology guidelines strongly recommend immediate initiation of antidotal therapy, as delayed treatment may still provide hepatoprotective benefit and limit progression to fulminant hepatic failure. In this case, due to the unavailability of methionine and fomepizole, specific antidotal therapy could not be administered, and management was therefore restricted to intensive supportive care. Even out of time limits, NAC was administered. The clinical course was complicated by hepatic, renal, and hemodynamic dysfunction, consistent with multi-organ involvement secondary to acute liver failure. Renal replacement therapy is generally indicated not only for metabolic acidosis, electrolyte disturbances (notably hyperkalemia), and severely reduced glomerular filtration rate (GFR < 15 mL/min), but also for uremic manifestations, including profound fatigue, altered mental status, and seizures, as well as for its potential contribution to toxin and metabolite clearance. However, in our patient, the indications for renal replacement therapy were not reached, therefore it was not initiated. Advanced extracorporeal liver support systems, such as single-pass albumin dialysis (SPAD) and the MARS, which may enhance hepatic detoxification and reduce circulating bilirubin, ammonia, and lactate levels, were not available in our setting. Consequently, referral to a specialized center for urgent liver transplantation in the context of acute liver failure was initiated. Supportive management in the intensive care unit was directed toward stabilization of hepatic function, renal impairment, and hemodynamic status, while preventing complications of liver failure, including coagulopathy, encephalopathy, hypoglycemia, and thermoregulatory instability. Oxygen therapy was administered via face mask at 3–5 L/min, with continuous capnography and serial arterial blood gas monitoring. Hemodynamic support included cautious volume resuscitation with Ringer’s lactate, recognizing its potential hypotonicity and the need to avoid exacerbation of intracranial pressure in the setting of hepatic encephalopathy. Metabolic acidosis was corrected with intravenous sodium bicarbonate (8.4% diluted in 5% glucose), with dosing guided by the standard formula: HCO3− deficit (mEq) = 0.5 × body weight (61 kg) × (target HCO3− (24 mEq/L) − measured HCO3−). Initially, 50% of the calculated deficit was administered, followed by reassessment and titration based on repeat arterial blood gas analysis. Electrolyte imbalances were carefully corrected using intravenous potassium chloride, calcium chloride, and magnesium sulfate with close laboratory monitoring guiding therapy. Strict temperature monitoring was maintained using a continuous skin probe, and hypothermia was actively prevented through warming blankets and warmed intravenous fluids, given its association with worsened coagulopathy and hemodynamic instability in liver failure. Hypoglycemia, a frequent consequence of impaired hepatic gluconeogenesis, was treated with 40% glucose and continuous monitoring. Coagulopathy, reflecting reduced hepatic synthesis of clotting factors, was managed with platelet transfusions, fresh frozen plasma, and vitamin K, guided by PT, INR, and clinical evidence of bleeding. Hepatic encephalopathy was addressed with lactulose to reduce ammonia absorption and production, along with gastrointestinal decontamination using neomycin and activated charcoal. Additional hepatoprotective measures included administration of vitamin E and silymarin, while ursodeoxycholic acid was used to support bile flow and manage hyperbilirubinemia. Overall, management focused on mitigating the systemic consequences of acute liver failure, including metabolic derangements, renal dysfunction, circulatory instability, and neurological complications, while arranging definitive treatment through liver transplantation.
Follow-up and outcome
Marked laboratory derangements were observed during the clinical course, with a peak AST of 11,688 U/L and ALT of 11,224 U/L, both recorded at day 3, accompanied by a profoundly elevated INR of 13.91 on the same day, reflecting severe hepatic injury and coagulopathy. Total bilirubin reached its maximum value of 35.65 mg/dL on day 22, indicating prolonged cholestasis. A nadir glycemia of 32 mg/dL was documented on day 6, consistent with significant metabolic impairment. Additional findings included marked leukocytosis, with white blood cell counts rising to 21,900 k/µL, progressive anemia with hemoglobin levels around 9–10 g/dL, and thrombocytopenia ranging between approximately 80,000 and 100,000 k/µL. Mild electrolyte disturbances were noted throughout the course, while renal function remained preserved. Notably, all microbiological cultures were negative, arguing against a superimposed infectious process. Despite these severe biochemical abnormalities, she showed progressive improvement with supportive care, including normalization of liver enzymes, improvement in coagulation parameters, and a gradual decline in bilirubin levels. The patient ultimately achieved complete clinical recovery. Tables 1–9 and Figures 1–9 illustrate the trends in transaminases, bilirubin, INR, glycemia, white and red blood cell counts, hemoglobin and hematocrit, and platelet count throughout hospital treatment.
 Click to view | Table 1. Transaminase Levels Over Time During Hospitalization |
Click to view | Table 2. Blood Bilirubin Levels Over Time During Hospitalization |
Click to view | Table 3. The INR Over Time During Hospitalization |
Click to view | Table 4. Blood Glucose Levels Over Time During Hospitalization |
Click to view | Table 5. WBC Count Over Time During Hospitalization |
Click to view | Table 6. RBC Count Over Time During Hospitalization |
Click to view | Table 7. HgB Levels Over Time During Hospitalization |
Click to view | Table 8. HCT Levels Over Time During Hospitalization |
Click to view | Table 9. PLT Count Over Time During Hospitalization |
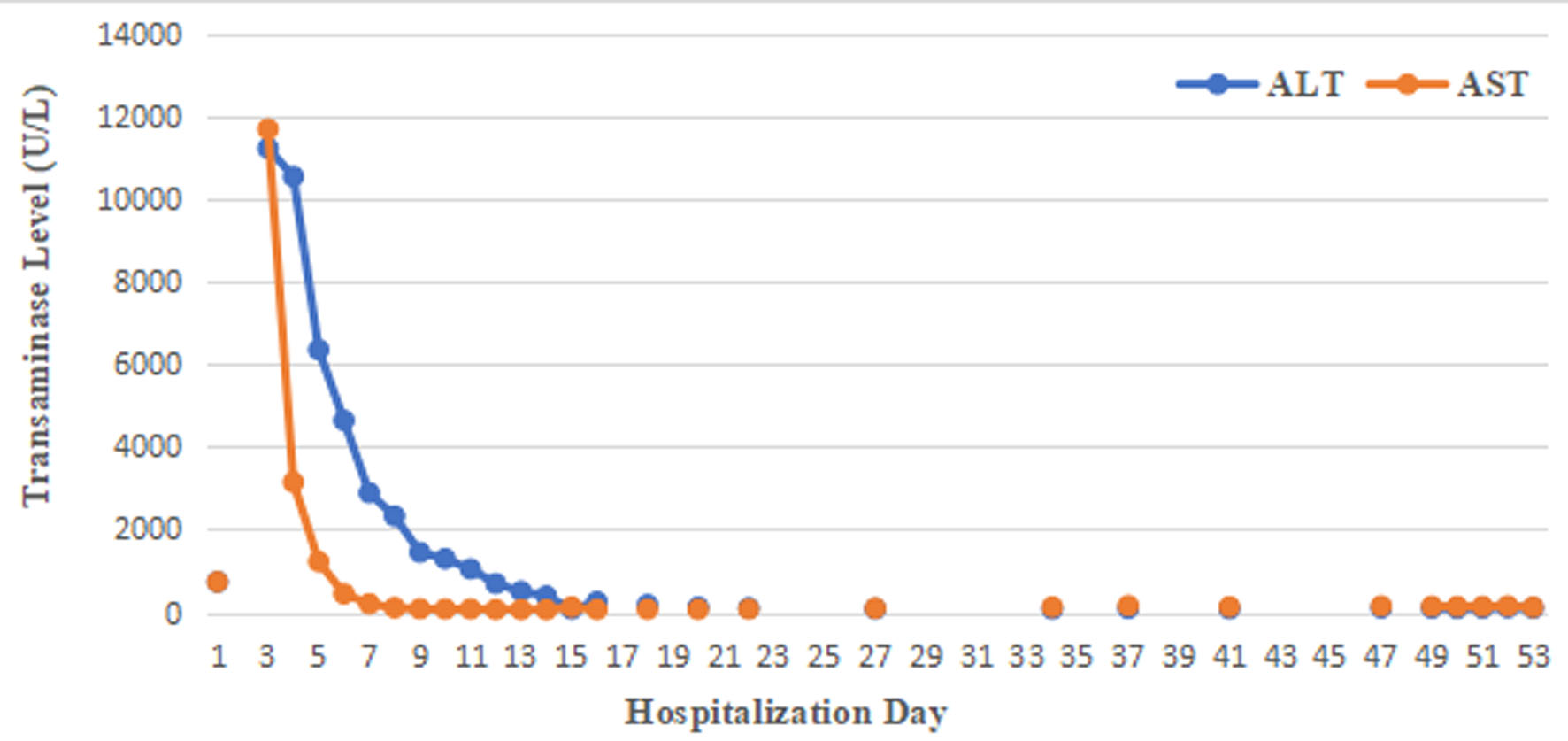 Click for large image | Figure 1. Transaminase levels over time during hospitalization. |
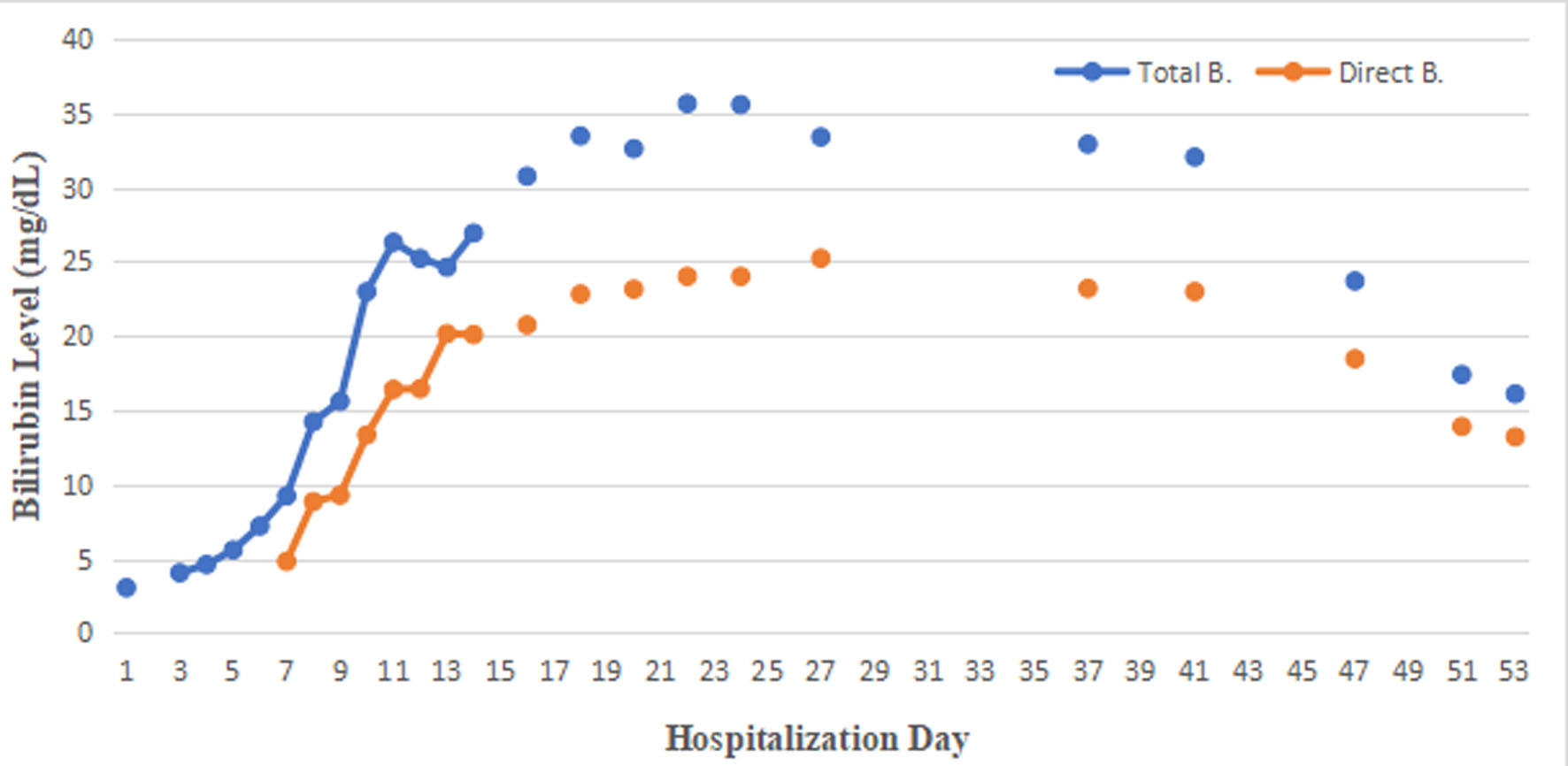 Click for large image | Figure 2. Blood bilirubin levels over time during hospitalization. |
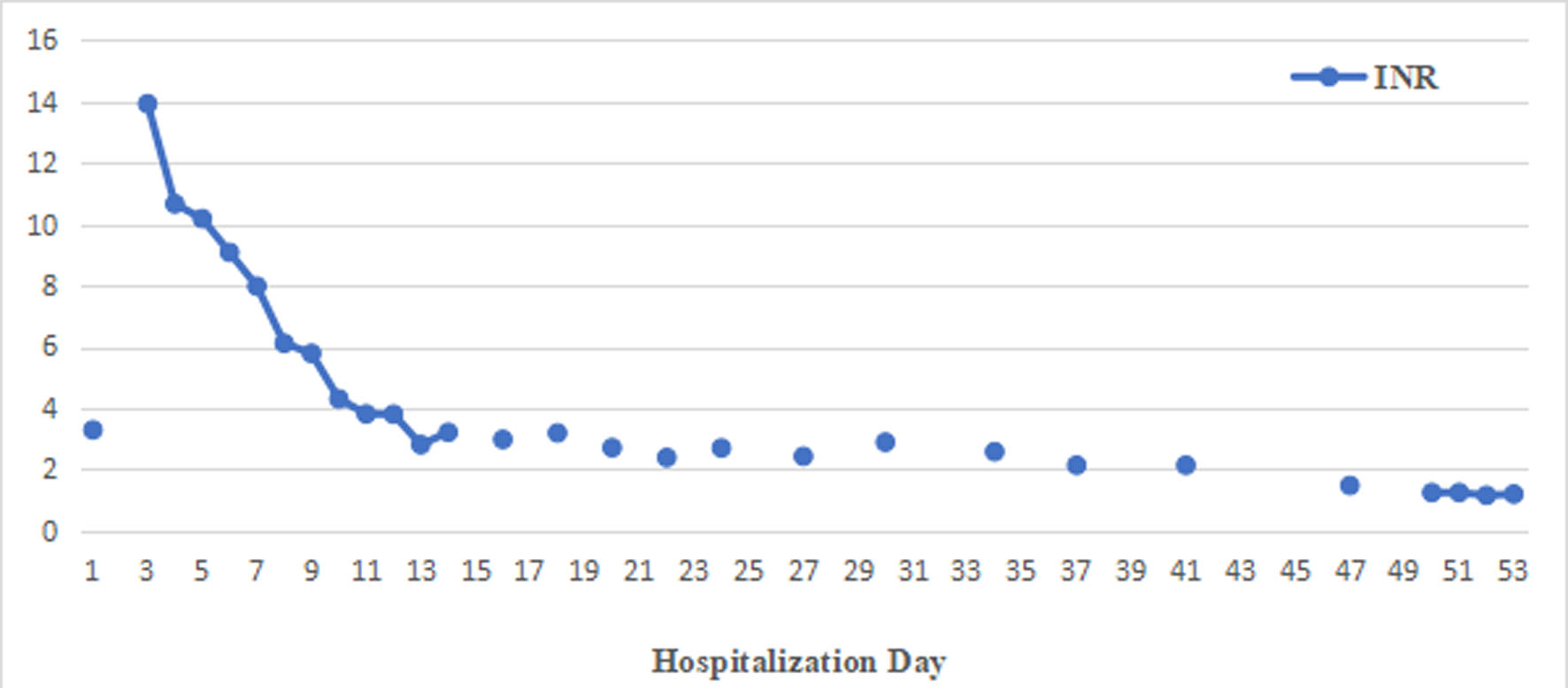 Click for large image | Figure 3. The international normalized ratio (INR) over time during hospitalization. |
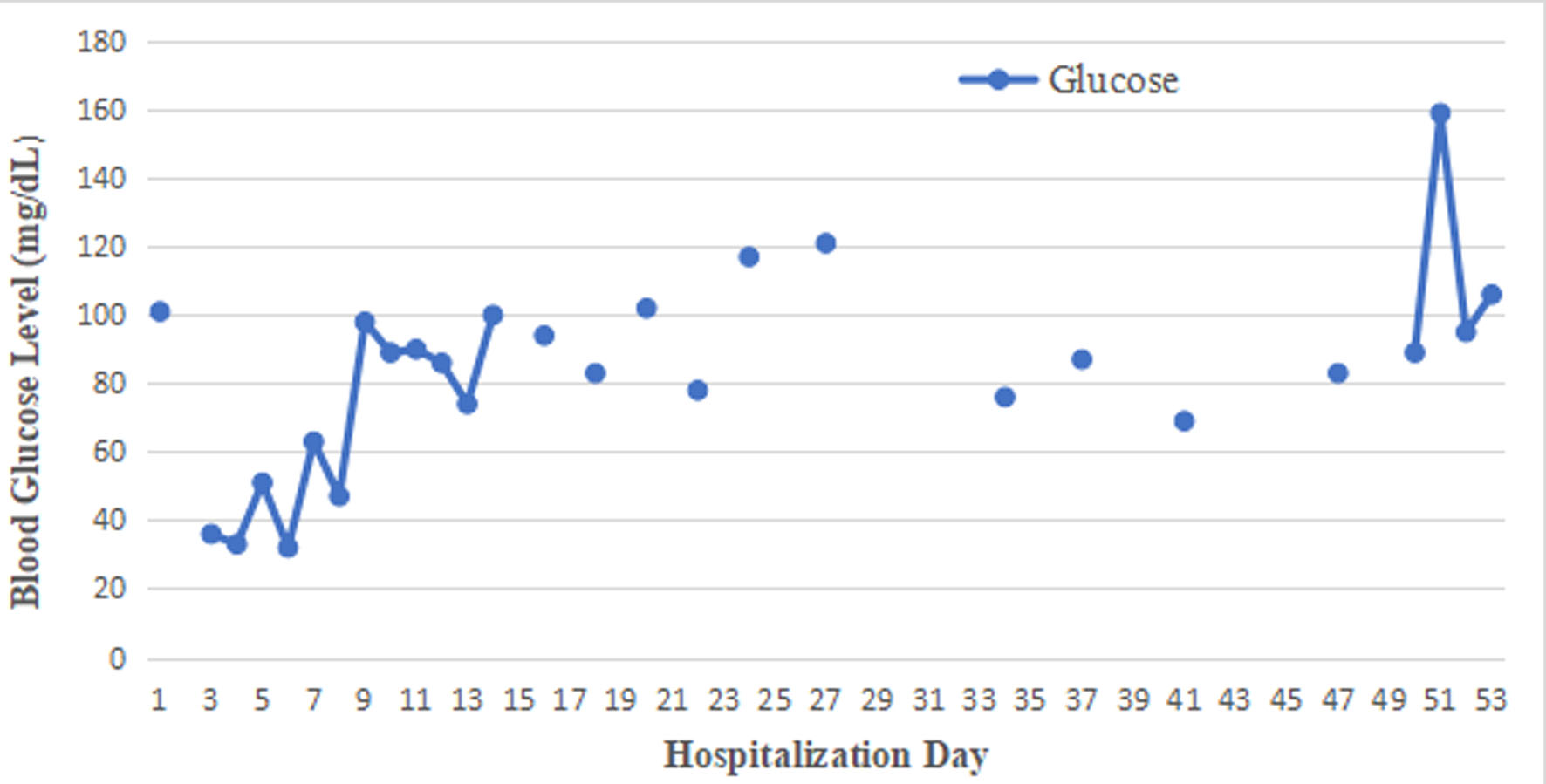 Click for large image | Figure 4. Blood glucose levels over time during hospitalization. |
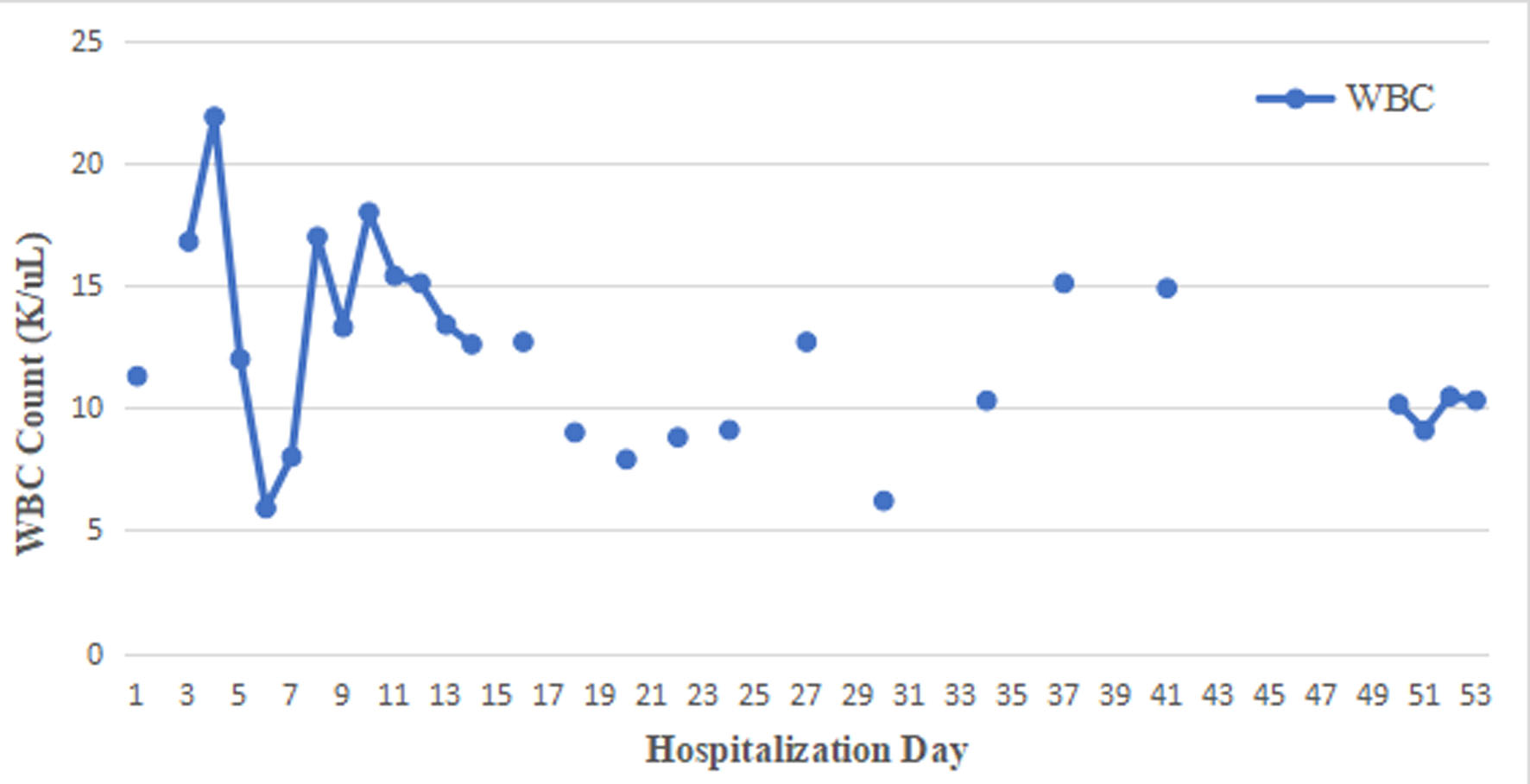 Click for large image | Figure 5. White blood cell (WBC) count over time during hospitalization. |
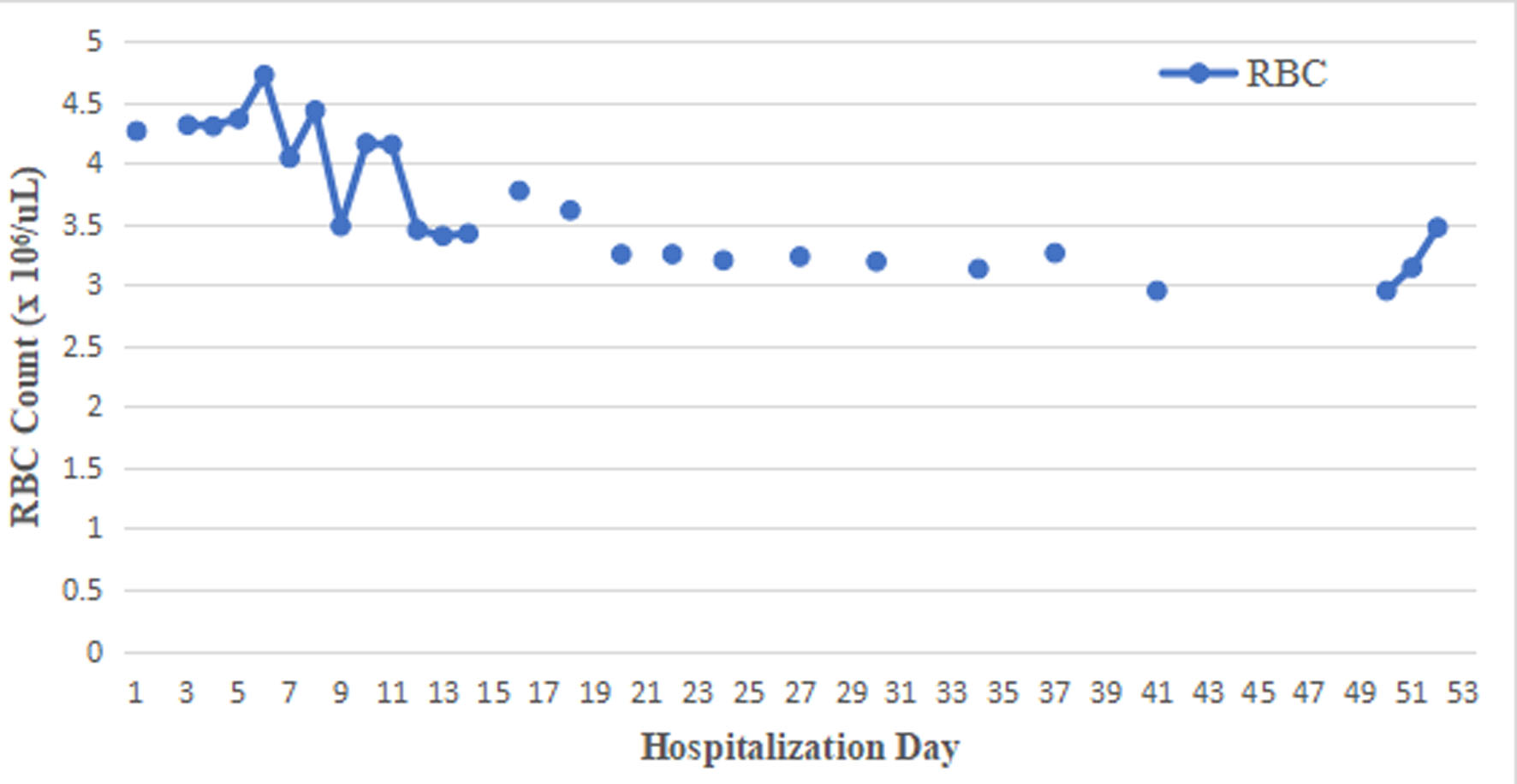 Click for large image | Figure 6. Red blood cell (RBC) count over time during hospitalization. |
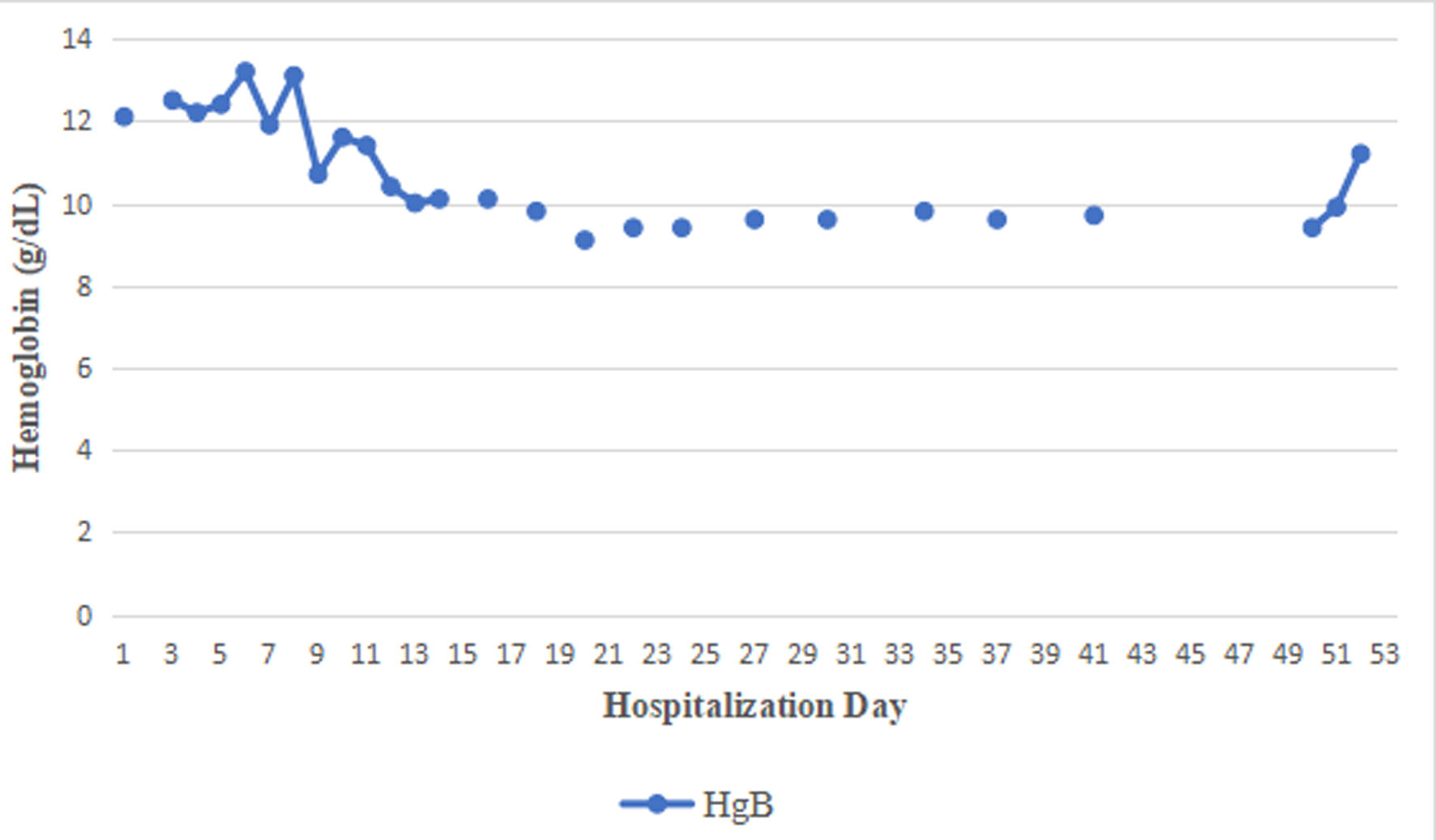 Click for large image | Figure 7. Hemoglobin levels over time during hospitalization. |
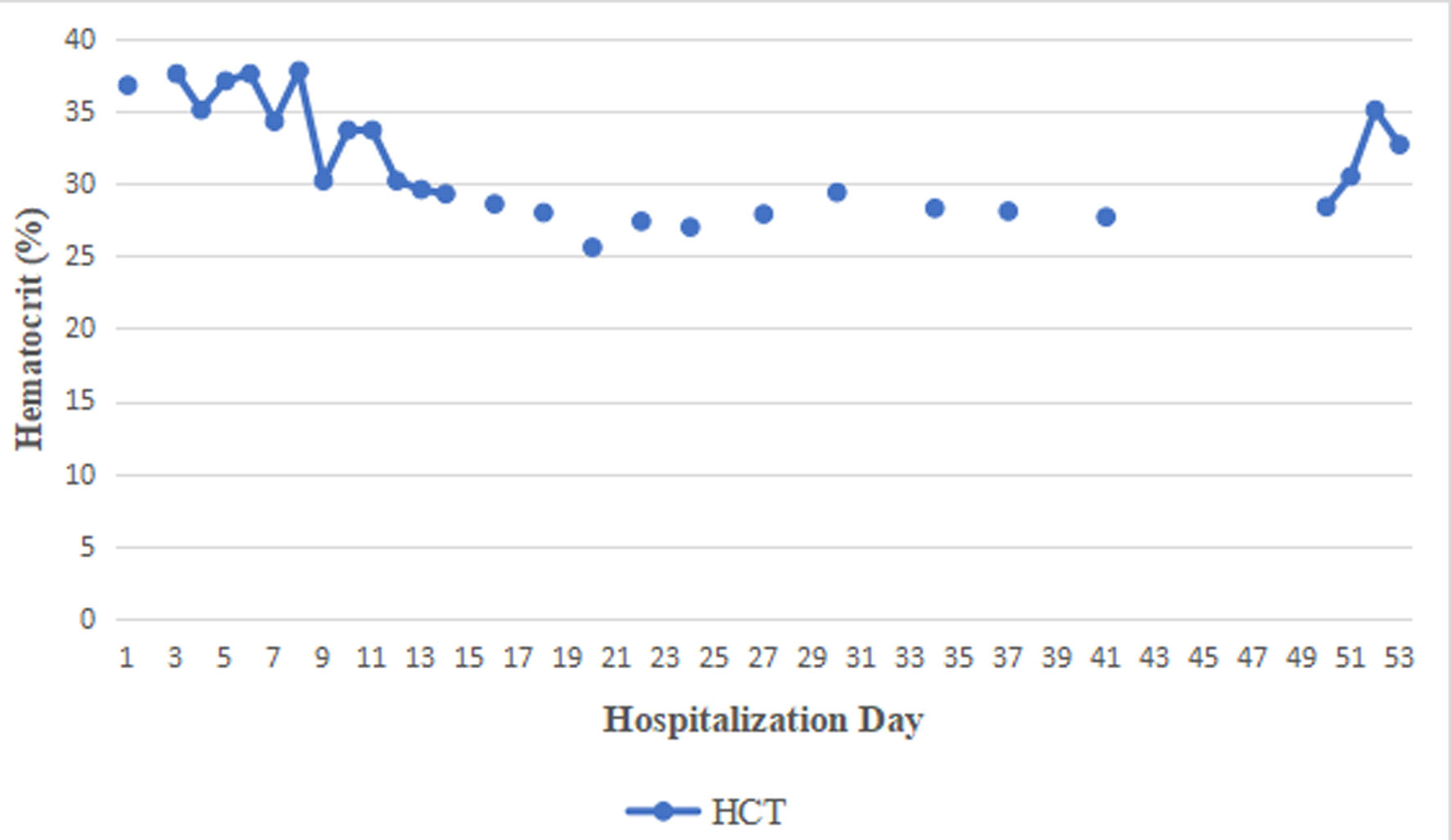 Click for large image | Figure 8. Hematocrit levels over time during hospitalization. |
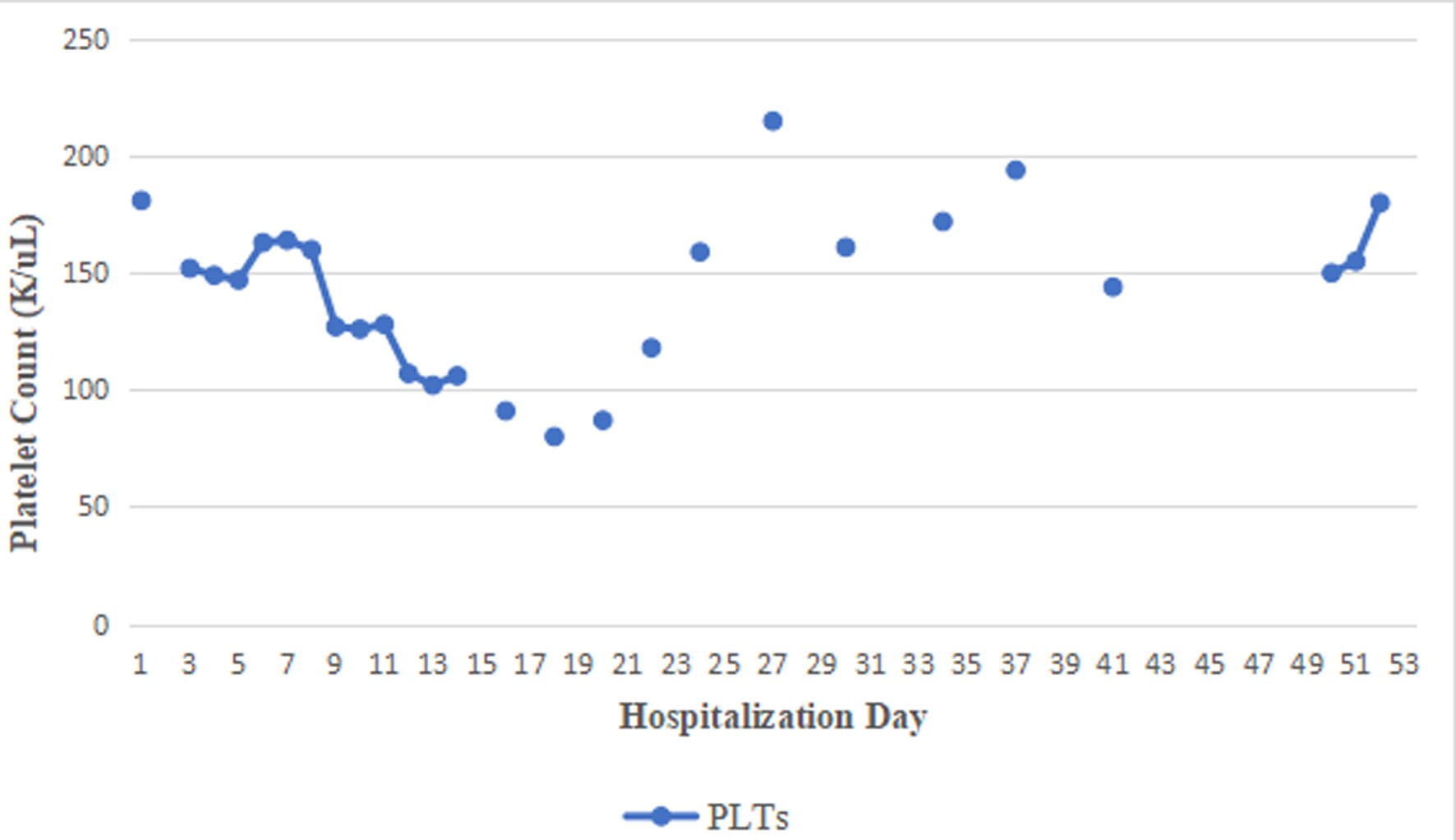 Click for large image | Figure 9. Platelet count over time during hospitalization. |
| Discussion | ▴Top |
In population-based studies, the incidence of acute overdose is estimated at approximately 21 cases per 100,000 persons per year, with around 5 per 100,000 requiring hospitalizations [3]. The burden remains considerable in high-income settings; in the United States alone, paracetamol toxicity accounts for nearly 56,000 emergency department visits and 2,600 hospitalizations each year [4]. In absolute numbers, it is responsible for roughly 500 deaths annually in the United States and 150–200 deaths per year in England and Wales, and it continues to represent a leading indication for liver transplantation worldwide [4]. Table 10 summarizes the four stages of acetaminophen-induced liver injury [5, 6]. The Service of Clinical Toxicology at the University Hospital Center “Mother Teresa,” Albania, admitted 46 patients with acetaminophen overdose and 19 with ibuprofen overdose in 2023, out of a total of 206 patients treated in the service. Elgingihy et al evaluated repeated exposure to paracetamol and ibuprofen in male albino mice, demonstrating hematological, histopathological, and molecular alterations with both agents. Ibuprofen was associated with more pronounced changes in blood indices, while each drug produced mild, dose-dependent structural alterations in organs such as the liver and kidneys without overt organ failure. At the molecular level, downregulation of tumor necrosis factor-α (TNF-α) and connexin 43 suggested early systemic effects. These findings indicate that even sub-chronic use at therapeutic levels may induce early biological changes, highlighting the need for cautious use and further long-term investigation [7]. Recent reports have described several antidotal strategies aimed at mitigating DILI, as reflected in European Association for the Study of the Liver (EASL) guidelines [8]. In DILI management, prompt discontinuation of the offending agent remains the primary intervention, as many cases improve spontaneously thereafter. The role of antidotes is limited: NAC is the principal evidence-based therapy, primarily indicated for acetaminophen hepatotoxicity and occasionally used in acute liver failure of other causes. For most drugs, specific antidotes are either unavailable or lack sufficient supporting evidence. Corticosteroids may be considered in selected immune-mediated cases, whereas ursodeoxycholic acid is not recommended routinely. When progression to acute liver failure occurs, management prioritizes supportive care and liver transplant evaluation, underscoring that, aside from NAC, treatment is largely supportive in nature [8]. Gartner et al investigated the clinical impact of fomepizole as an adjunct to standard NAC therapy in high-risk acetaminophen overdose. The addition of fomepizole, an inhibitor of cytochrome P450 2E1 (CYP2E1), was associated with improved outcomes, including reduced progression to severe hepatotoxicity and acute liver failure. Patients receiving combination therapy demonstrated more favorable trends in liver enzyme evolution and overall clinical course compared with standard treatment alone. These results suggest that fomepizole may limit toxic metabolite formation and provide benefit in selected high-risk cases, although further prospective data are required to define its role [9]. Nogue-Xarau et al reviewed five decades of clinical experience with NAC, emphasizing its transformative effect on the prognosis of acetaminophen poisoning. NAC replenishes glutathione stores, enhances detoxification of the toxic metabolite N-acetyl-4-benzoquinone imine (NAPQI), and exerts antioxidant and anti-inflammatory actions. Early administration markedly reduces hepatotoxicity and mortality, establishing NAC as the cornerstone of treatment. Over time, dosing regimens and routes of administration have been refined to improve safety and tolerability. Nonetheless, challenges persist in late-presenting cases and in optimizing treatment for high-risk patients, highlighting the need for ongoing refinement of therapeutic strategies [10]. Nakatsu et al conducted a systematic review and meta-analysis comparing two-bag versus traditional three-bag intravenous acetylcysteine regimens in paracetamol poisoning. Their findings show that the two-bag regimen achieves comparable efficacy in preventing hepatotoxicity while significantly reducing adverse reactions, particularly anaphylactoid events, and simplifying administration. It was also associated with fewer interruptions and medication errors. Overall, the study supports the two-bag protocol as a safe and effective alternative with practical advantages in clinical settings [11]. Muriel et al described methionine as a hepatoprotective agent owing to its central role in hepatic metabolism and antioxidant defense. As a precursor of S-adenosylmethionine (SAMe) and glutathione, it contributes to reducing oxidative stress, enhancing detoxification, and maintaining redox balance. Methionine also supports lipid metabolism, helping to limit hepatic steatosis, and exerts anti-inflammatory and antifibrotic effects through modulation of cytokine production and inhibition of stellate cell activation. Overall, it represents a potentially valuable therapeutic strategy in liver disease through combined metabolic and regulatory effects [12]. The Rumack–Matthew nomogram is a widely used clinical tool for assessing the risk of hepatotoxicity after acute acetaminophen overdose and for guiding the initiation of NAC therapy [13]. However, its applicability is limited to single acute ingestions with a clearly known time of exposure, and it is considered valid only when serum paracetamol concentrations are measured between 4 and 24 h after ingestion [14]. In our case, the patient presented more than 48 h after the reported ingestion, rendering the Rumack–Matthew nomogram clinically unhelpful. Nevertheless, NAC therapy was administered despite the delayed presentation because of the strong clinical and laboratory evidence of significant acetaminophen toxicity. Even when initiated beyond the conventional early window, antidotal therapy may still confer hepatoprotective effects, attenuate ongoing injury, and reduce progression to fulminant hepatic failure. This approach highlights that, despite limitations in available antidotes for DILI, NAC may remain beneficial even in late-presenting cases [15]. MARS is an advanced liver support modality used in severe liver failure, including DILI, when conventional therapy is insufficient. It employs albumin dialysis to remove both albumin-bound and water-soluble toxins, such as bilirubin and bile acids, thereby improving hepatic encephalopathy, hemodynamic status, and overall toxin burden while allowing time for hepatic recovery. Although it does not replace the liver’s synthetic or metabolic functions, MARS can serve as a bridge to recovery or transplantation in fulminant hepatic failure. Its use is generally limited to critically ill patients in specialized centers where liver dysfunction progresses despite optimal supportive care [16–18]. As MARS is not available in Albania, our patient was managed exclusively with supportive therapy, focusing on hemodynamic stabilization, correction of metabolic disturbances, and close monitoring of liver and renal function to preserve organ perfusion and facilitate spontaneous recovery. Although MARS represents a dedicated extracorporeal liver support therapy, continuous renal replacement therapy (CRRT) and intermittent hemodialysis are commonly used as supportive alternatives in centers where MARS is unavailable. In Albania, CRRT and intermittent hemodialysis are routinely available and may provide metabolic and renal support in acute liver failure, although they do not fully replicate the albumin-bound toxin clearance achieved by MARS. In our case, however, the patient presented more than 48 h after ingestion, when hepatic injury was already established, limiting the potential benefit of extracorporeal toxin removal therapies. Furthermore, renal impairment and metabolic acidosis were not severe, while hemodynamic status and urinary output remained preserved throughout hospitalization. Patients with acute liver failure require intensive care with continuous monitoring of vital signs, neurological status, and laboratory parameters, along with careful management of fluids, electrolytes, and acid–base balance. Hemodynamic support with fluids and vasopressors, prevention and treatment of cerebral edema, selective correction of coagulopathy, renal support including renal replacement therapy when indicated, infection surveillance with timely treatment, metabolic and nutritional optimization, and respiratory support all constitute essential components of care. The goal of supportive management is to stabilize organ function, prevent complications, and maintain metabolic homeostasis while definitive therapies, including liver transplantation, are evaluated [19]. Table 11 summarizes general supportive treatment strategies [20]. Supportive care in acute liver failure is inherently multisystem, aiming to stabilize hemodynamics,preventcomplications, and preserve organ function while definitive interventions, including transplantation, are considered. Fluid management requires careful assessment and guided resuscitation with balanced crystalloids, avoiding both hypovolemia and overload [20]. Noradrenaline is the vasopressor of choice for fluid-refractory hypotension, maintaining adequate mean arterial pressure and organ perfusion while limiting ischemic risk [21]. Cerebral edema, a major determinant of morbidity, is managed through minimal stimulation, gentle suctioning, strict glucose control, and electrolyte optimization, targeting serum sodium levels of 145–155 mEq/L with hypertonic saline or mannitol when indicated [22, 23]. NAC offers hepatoprotective benefits in both paracetamol and non-paracetamol acute liver failure, improving short-term outcomes. Early initiation of CRRT supports ammonia clearance, corrects metabolic disturbances, and assists in fluid balance [24]. Mild therapeutic hypothermia may reduce cerebral edema and metabolic demand, although supporting evidence remains limited. Mechanical ventilation is reserved for advanced encephalopathy to protect the airway and manage intracranial pressure [25]. Attention to phosphate balance supports neurological recovery, while treatments commonly used for hyperammonemia in chronic liver disease are ineffective in the acute setting [26]. In our patient, hemodynamic stability was achieved through cautious fluid resuscitation with Ringer’s lactate and targeted vasopressor use, in line with recommendations to avoid both hypovolemia and fluid overload. Cerebral edema was managed with close monitoring, glucose control, and electrolyte optimization, while advanced measures such as hypertonic saline or mannitol were reserved for clear indications. NAC was administered despite delayed presentation, reflecting guideline recognition that late treatment may still provide benefit. Additional supportive measures included oxygen therapy, fluid management, temperature control, and targeted correction of coagulopathy and hypoglycemia, consistent with intensive care unit-level monitoring and complication prevention. Limitations were primarily related to resource availability: advanced liver support systems such as MARS and adjunctive antidotes like methionine or fomepizole were not accessible, necessitating reliance on conventional supportive care while arranging transplant evaluation. Overall, management adhered closely to EASL-recommended principles, adapted to local constraints and delayed presentation, ultimately stabilizing multiorgan dysfunction and enabling complete clinical recovery.
Click to view | Table 10. Acetaminophen Liver Damage Stages [5, 6] |
Click to view | Table 11. General Supportive Treatment’s Modalities [18] |
Conclusions
Comprehensive supportive care including correction of hepatic, renal, central nervous system, metabolic, and coagulation abnormalities successfully prevented life-threatening complications, halted progression to irreversible organ damage, and provided sufficient time for hepatic recovery, even in the absence of specific antidotal therapy.
Learning points
Combined overdose with acetaminophen and ibuprofen can lead to severe multi-organ toxicity, particularly when presentation is delayed.
NAC should be administered even in delayed presentations, as it may still provide hepatoprotective effects and improve outcomes.
In resource-limited settings where antidotes and advanced therapies are unavailable, meticulous supportive care becomes the cornerstone of management and may be lifesaving.
Comprehensive supportive management must address hepatic failure, metabolic acidosis, coagulopathy, renal dysfunction, and hypoglycemia, with close monitoring in an intensive care setting.
Advanced extracorporeal liver support systems such as MARS can serve as a bridge to recovery or transplantation but are not universally accessible.
Even in severe acute liver failure with extreme biochemical derangements, favorable outcomes may be possible without liver transplantation when complications are effectively controlled.
This case underscores the critical importance of early recognition, aggressive supportive therapy, and sustained monitoring, especially in delayed presentations and low-resource environments.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Informed consent has been obtained.
Author Contributions
Manuscript writing: AD and RD; literature searching: ES, VE, GH, AA, and MN; language editing: RD, EN, KL, AC, and FC.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Chidiac AS, Buckley NA, Noghrehchi F, Cairns R. Paracetamol (acetaminophen) overdose and hepatotoxicity: mechanism, treatment, prevention measures, and estimates of burden of disease. Expert Opin Drug Metab Toxicol. 2023;19(5):297-317.
doi pubmed - Park BK, Dear JW, Antoine DJ. Paracetamol (acetaminophen) poisoning. BMJ Clin Evid. 2015;2015:2101.
pubmed - Bond GR, Hite LK. Population-based incidence and outcome of acetaminophen poisoning by type of ingestion. Acad Emerg Med. 1999;6(11):1115-1120.
doi pubmed - Rajaram P, Subramanian R. Management of Acute Liver Failure in the Intensive Care Unit Setting. Clin Liver Dis. 2018;22(2):403-408.
doi pubmed - Schaffer DH, Murray BP, Khazaeni B. Acetaminophen toxicity. In: StatPearls. Treasure Island (FL) ineligible companies. 2026.
pubmed - Saccomano SJ. Acute acetaminophen toxicity in adults. Nurse Pract. 2019;44(11):42-47.
doi pubmed - Elgingihy SM, Elmaghraby AM, Mustafa YA, Elseehy MA, Haggag AS, Abdel-Rahman SM. Toxicological evaluation of paracetamol and ibuprofen: genetic and hematological alterations in male albino mice. BMC Pharmacol Toxicol. 2026;27(1).
doi pubmed - Brennan PN, Cartlidge P, Manship T, Dillon JF. Guideline review: EASL clinical practice guidelines: drug-induced liver injury (DILI). Frontline Gastroenterol. 2022;13(4):332-336.
doi pubmed - Gartner HT, Simmons RE, Stott M, Perez V, Crespo J, Allison B, Howard A, et al. Clinical impact of fomepizole as an adjunct therapy in high-risk acetaminophen overdose. Am J Emerg Med. 2026;104:128-134.
doi pubmed - Nogue-Xarau S, Martinez-Sanchez L, Garcia-Pelaez M, Fernandez de Gamarra-Martinez E, Pi-Sala N, Gispert-Ametller A, Salgado-Garcia E, et al. N-acetylcysteine: 50 years since the discovery of an antidote that has changed the prognosis of acetaminophen poisoning. Farm Hosp. 2026;50(3):162-166.
doi pubmed - Nakatsu L, Lopez JR, Garcia CM, Cherian M, Nash J, Tofighi D, Seifert SA, et al. Comparison of two-bag and three-bag acetylcysteine regimens in the treatment of paracetamol poisoning: a systematic review and meta-analysis. Clin Toxicol (Phila). 2025;63(3):155-165.
doi pubmed - Muriel P, Vargas-Pozada EE, Marquez-Quiroga LV, Ramos-Tovar E. Potential therapeutic strategies for steatosis, oxidative stress, inflammation, and fibrosis in liver disease. Int J Mol Sci. 2026;27(6):2546.
doi pubmed - Rumack BH, Matthew H. Acetaminophen poisoning and toxicity. Pediatrics. 1975;55(6):871-876.
pubmed - Dart RC, Mullins ME, Matoushek T, Ruha AM, Burns MM, Simone K, Beuhler MC, et al. Management of acetaminophen poisoning in the US and Canada: a consensus statement. JAMA Netw Open. 2023;6(8):e2327739.
doi pubmed - Alhammad AM, Alajmi G, Alkhodair A, Mansy WH, Aljawadi MH, Aljadeed R, Alshammari R, et al. Patterns of acetaminophen toxicity among patients with low-risk serum concentrations. J Int Med Res. 2024;52(7):3000605241260362.
doi pubmed - Podoll AS, DeGolovine A, Finkel KW. Liver support systems—a review. ASAIO J. 2012;58(5):443-449.
doi pubmed - Mielnicki W, Dyla A, Karczewski M. Clinical effectiveness of MARS treatment - multidirectional analysis of positive clinical response to treatment. Clin Exp Hepatol. 2019;5(4):271-278.
doi pubmed - Stange J, Mitzner SR, Risler T, Erley CM, Lauchart W, Goehl H, Klammt S, et al. Molecular adsorbent recycling system (MARS): clinical results of a new membrane-based blood purification system for bioartificial liver support. Artif Organs. 1999;23(4):319-330.
doi pubmed - European Association for the Study of the Liver. EASL Clinical Practical Guidelines on the management of acute (fulminant) liver failure.J Hepatol. 2017;66(5):1047-1081.
doi pubmed - Kumar R, Bhatia V. Structured approach to treat patients with acute liver failure: a hepatic emergency. Indian J Crit Care Med. 2012;16(1):1-7.
doi pubmed - Aziz R, Price J, Agarwal B. Management of acute liver failure in intensive care. BJA Educ. 2021;21(3):110-116.
doi pubmed - Scott TR, Kronsten VT, Hughes RD, Shawcross DL. Pathophysiology of cerebral oedema in acute liver failure. World J Gastroenterol. 2013;19(48):9240-9255.
doi pubmed - Fernandez J, Bassegoda O, Toapanta D, Bernal W. Acute liver failure: a practical update. JHEP Rep. 2024;6(9):101131.
doi pubmed - Fisher C, Warrillow S. Continuous renal replacement therapy in acute liver failure. World J Crit Care Med. 2026;15(1):110552.
doi pubmed - Karcz M, Bankey B, Schwaiberger D, Lachmann B, Papadakos PJ. Acute respiratory failure complicating advanced liver disease. Semin Respir Crit Care Med. 2012;33(1):96-110.
doi pubmed - Bajaj JS, Jakab SS, Jesudian AB, Rahimi RS, Duarte-Rojo A, Chen PH, Wong RJ, et al. ACG clinical guideline: hepatic encephalopathy. Am J Gastroenterol. 2026;121(3):588-618.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.