| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://jmc.elmerpub.com |
Case Report
Volume 17, Number 8, August 2026, pages 385-393

Emergency Laparoscopic Appendectomy in a High-Risk Cardiac Patient With Severe Left Main Coronary Artery Disease on Dual Antiplatelet Therapy
Blerim Arapia, Alma Canib, Rudin Domib, j, Gentian Hutic, Asead Abdylic, Krenar Lilajb, Filadelfo Coniglioned, Mustafa Bajraktarie, Rinard Kortocie, Majlinda Nacob, Arjana Sinaf, Migena Vargug, Ergita Nelajh, Vedat Eljezii
aDepartment of Anesthesia and Intensive Care, Hygeia International Hospital, Tirana, Albania
bDepartment of Surgery, University of Medicine, Tirana, Albania
cDepartment of Anesthesia and Intensive Care, American Hospital 3, Tirana, Albania
dDepartment of Clinical Science and Translational Medicine, Tor Vergata University of Rome, Rome, Italy
eDepartment of Anesthesia and Intensive Care, American Hospital 2, Tirana, Albania
fImaging Service, Wellness Albania Clinic, Tirana, Albania
gDepartment of Infectious Diseases, University of Medicine, Tirana, Albania
hDepartment of Internal Medicine, University of Medicine, Tirana, Albania
iDepartment of Perioperative Medicine, CHU Gabriel-Montpied, Clermont-Ferrand, France
jCorresponding Author: Rudin Domi, Department of Surgery, Service of Anesthesia and Intensive Care, University of Medicine, Tirana, Albania
Manuscript submitted March 25, 2026, accepted May 21, 2026, published online July 1, 2026
Short title: Emergency Surgery in High-Risk CAD
doi: https://doi.org/10.14740/jmc5327
| Abstract | ▴Top |
Emergency noncardiac surgery in patients with advanced coronary artery disease and recent coronary stent implantation poses a substantial anesthetic challenge. Clinicians must carefully balance the heightened risk of perioperative bleeding associated with continued dual antiplatelet therapy against the potentially catastrophic risk of stent thrombosis if such therapy is interrupted. We described the perioperative management of a 68-year-old man with severe multivessel coronary artery disease, critical left main stenosis, impaired left ventricular function, and recent coronary stenting, who required emergency laparoscopic appendectomy for perforated appendicitis. General anesthesia was administered with comprehensive invasive hemodynamic monitoring and tailored vasopressor support. The procedure was completed successfully, and the postoperative course was uneventful. This case underscored the feasibility of proceeding with emergency laparoscopic abdominal surgery without interruption of dual antiplatelet therapy in a patient with high-risk coronary anatomy, including left main disease. It highlighted a pragmatic, individualized anesthetic strategy integrating advanced hemodynamic monitoring, goal-directed support, and close multidisciplinary coordination, offering practical insight into managing the competing risks of bleeding and stent thrombosis in time-critical surgical settings.
Keywords: Anesthesia; Coronary stents; Coronary artery disease; Dual antiplatelet therapy; Emergent surgery
| Introduction | ▴Top |
Patients with advanced coronary artery disease (CAD) who require urgent noncardiac surgery represent a particularly high-risk population, facing significant challenges from both cardiac and bleeding complications [1]. The presence of recent coronary stent implantation further increases perioperative vulnerability. Interrupting dual antiplatelet therapy (DAPT) to reduce bleeding risk can precipitate acute stent thrombosis, which is often fatal, whereas continuing DAPT increases the likelihood of significant perioperative bleeding, particularly in intra-abdominal procedures [2, 3]. These patients are also highly susceptible to myocardial ischemia, arrhythmias, and hemodynamic instability during surgery due to impaired coronary perfusion, reduced ventricular function, and stress response associated with emergency procedures [4]. Emergent conditions such as perforated appendicitis compound these risks, leaving no opportunity to safely delay surgery.
Guidelines from major societies provide structured recommendations to navigate these complex scenarios. The American College of Cardiology (ACC) advises a comprehensive preoperative risk assessment that considers recent coronary interventions, stent type and timing, left ventricular function, and functional capacity. Elective surgery is generally deferred for at least 30 days after bare-metal stent placement and 6 months after drug-eluting stent implantation to reduce the risk of stent thrombosis. In urgent or emergent situations, ACC guidance emphasizes continuation of DAPT whenever feasible and close multidisciplinary coordination to balance the competing risks of bleeding and thrombosis [5].
Similarly, the American Heart Association (AHA) highlights individualized risk stratification and careful perioperative planning. Noninvasive testing, such as stress evaluation or imaging, may be appropriate in selected high-risk patients if time allows, but in emergencies, the AHA recommends maintaining DAPT whenever possible. Collaboration among cardiologists, anesthesiologists, and surgeons is crucial to optimize hemodynamic management, minimize bleeding risk, and prevent cardiac complications [6].
The European Society of Cardiology (ESC) provides detailed recommendations for patients with recent coronary stents undergoing noncardiac surgery. The ESC guidelines stress deferring elective procedures according to stent type, 30 days for bare-metal stents and 6 months for drug-eluting stents, and continuing DAPT in high-risk patients when possible. Perioperative risk stratification should consider coronary anatomy, ventricular function, and the urgency of surgery, with invasive hemodynamic monitoring and goal-directed therapy recommended for high-risk cases, particularly when emergent surgery cannot be delayed [7].
This report presents the successful anesthetic management of a 68-year-old patient with severe multivessel CAD, critical left main stenosis, recent coronary stenting, and ongoing DAPT who required emergency laparoscopic appendectomy for perforated appendicitis.
The case demonstrates that emergency minimally invasive abdominal surgery can be safely performed in patients with high-risk coronary anatomy without interrupting DAPT, a scenario that remains scarcely addressed in the current literature. Unlike most previous reports, which focus on elective surgeries or theoretical recommendations, this case illustrates the practical challenges of balancing bleeding and thrombotic risks in an urgent clinical setting. By applying a physiology-driven, multidisciplinary strategy that integrates established guideline recommendations with individualized perioperative care, this report may provide a useful clinical example for the management of urgent noncardiac surgery in patients with recent stents.
| Case Report | ▴Top |
Investigations
A 68-year-old man presented with a 4- to 5-day history of abdominal pain, initially localized to the right posterior abdomen and later migrating to the right iliac fossa, with associated localized guarding. Clinically, the patient was initially suspected of having appendicitis, and a routine abdominal ultrasound was performed as the first-line imaging modality. However, the definitive diagnosis was established by computed tomography (CT) scan, which confirmed acute appendicitis and accurately defined the stage of disease, including perforation and advanced inflammatory involvement. In this high-risk patient, CT imaging was essential not only for diagnostic confirmation but also for assessment of disease severity and for supporting the decision that urgent surgical intervention was necessary (Fig. 1). Preoperative evaluation revealed an extremely high-risk cardiovascular profile. The patient had known triple-vessel CAD, including approximately 85% left main coronary artery stenosis, complete right coronary artery occlusion with collateral retrograde flow from the left anterior descending artery, and severe (90%) left circumflex artery stenosis. One month earlier, he had undergone stenting of the left anterior descending and D1 arteries (Fig. 2) and remained on DAPT with prasugrel 10 mg and aspirin 100 mg daily. A prior circumflex stent had been placed 15 years earlier, and coronary artery bypass grafting was already planned.
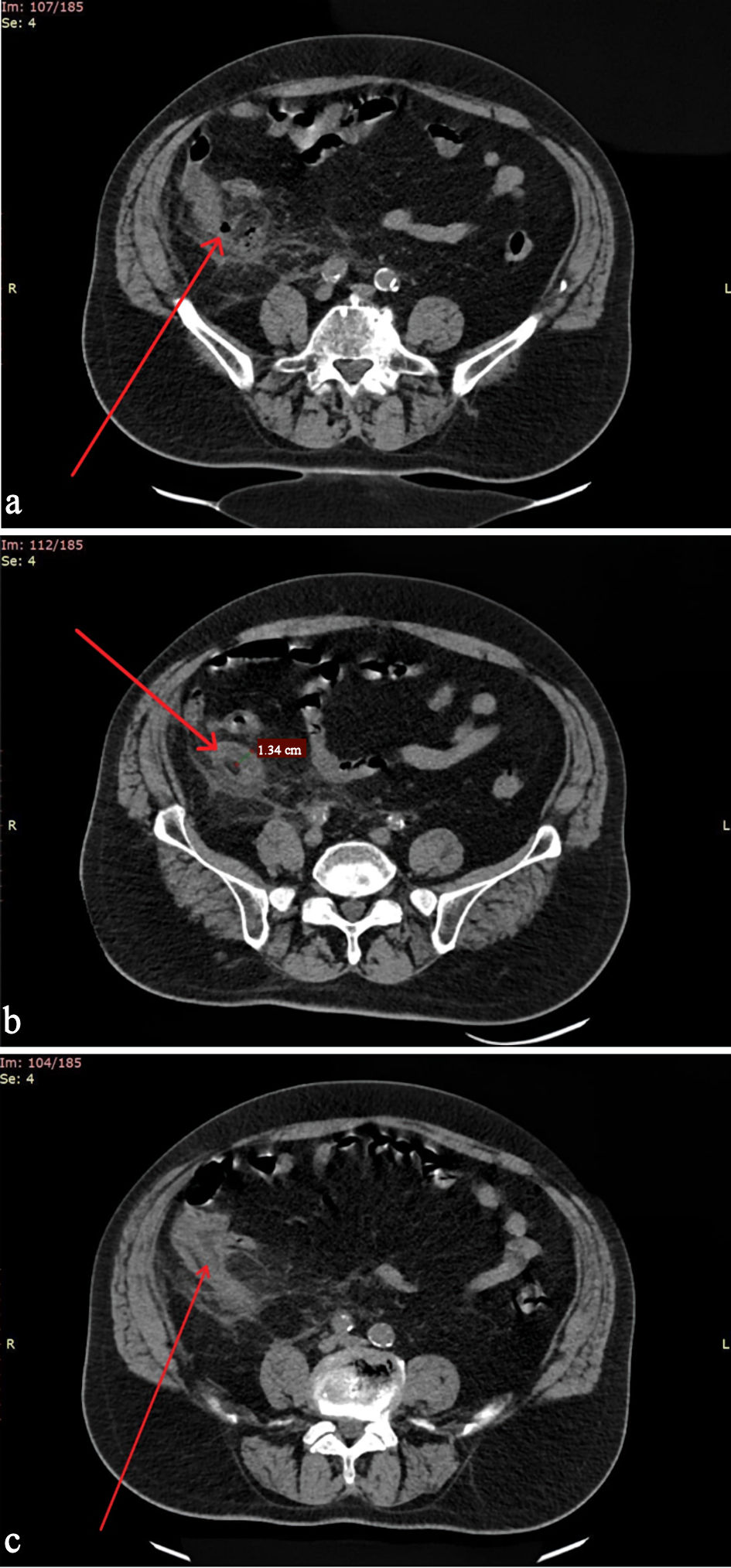 Click for large image | Figure 1. Abdominal CT scans demonstrating a perforated and severely inflamed appendix with appendiceal wall thickening and evidence of structural destruction (arrows). (a) Perforated appendix with structural destruction. (b) Marked appendiceal inflammation with increased wall thickness. (c) Additional axial view demonstrating perforation and inflammatory changes. CT: computed tomography. |
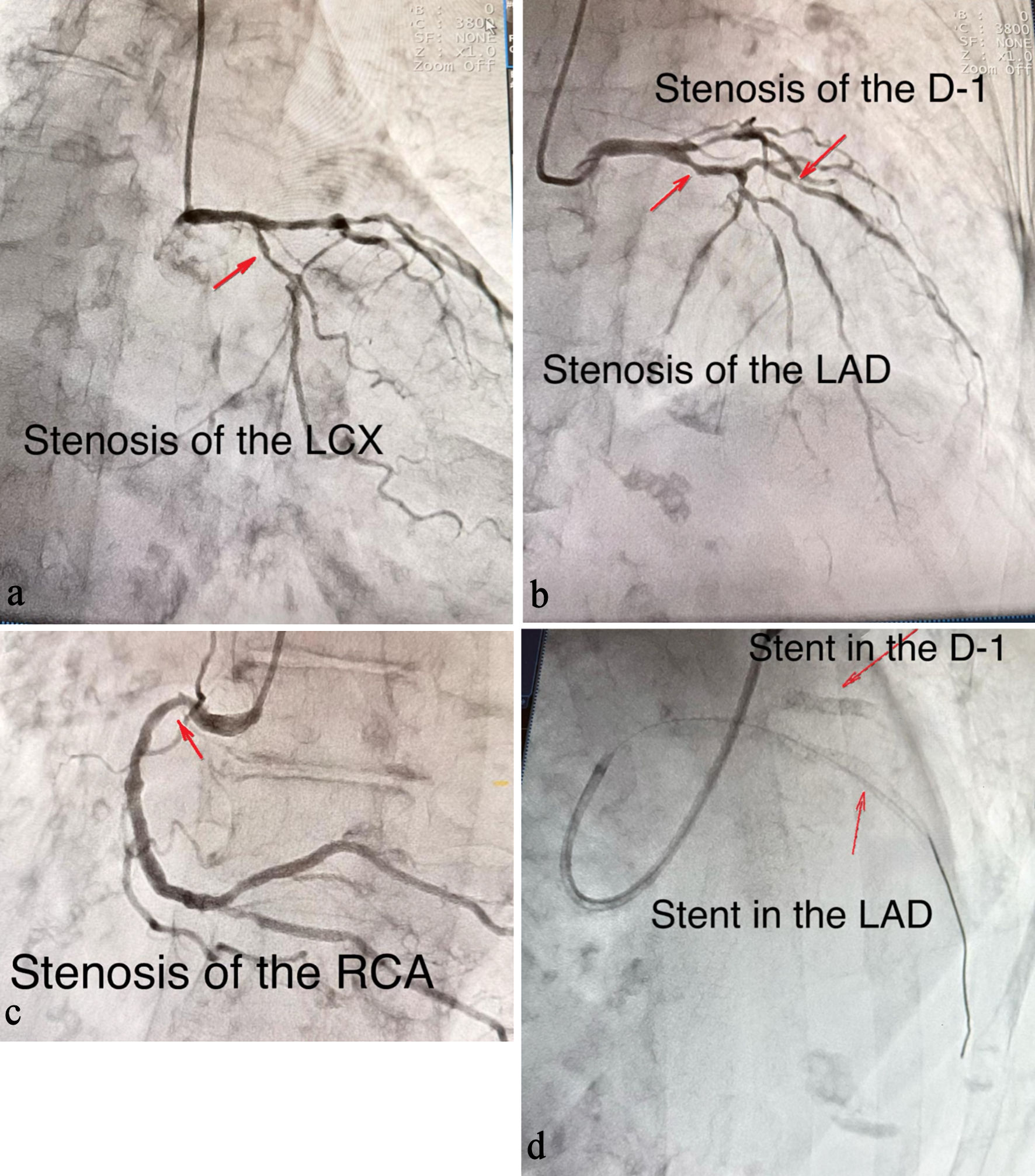 Click for large image | Figure 2. Coronary angiography and post-intervention findings. (a) Stenosis of the left circumflex artery (LCX). (b) Stenosis of the left anterior descending (LAD) and first diagonal (D-1) arteries. (c) Stenosis of the right coronary artery (RCA). (d) Final angiographic result after percutaneous coronary intervention and balloon angioplasty demonstrating stent placement in the LAD and D-1 arteries. |
Preoperative transthoracic echocardiography demonstrated severe left ventricular dysfunction with an ejection fraction of 30%, moderate mitral regurgitation, and marked left ventricular dilation (end-diastolic diameter 58 mm), consistent with advanced chronic heart failure; previously documented ejection fraction values ranged between 35% and 40%. Additional comorbidities included insulin-treated diabetes mellitus and arterial hypertension treated with bisoprolol and valsartan, while furosemide 25 mg daily was prescribed for heart failure management.
Objective perioperative risk stratification further confirmed the patient’s critical status. The Revised Cardiac Risk Index (RCRI) was 3 points and American Society of Anesthesiologists (ASA) Physical Status IV-E, based on ischemic heart disease, congestive heart failure, and insulin-treated diabetes mellitus, corresponding to a markedly increased risk of major perioperative cardiac complications during emergency surgery.
Diagnosis
The patient was diagnosed with perforated appendicitis with localized peritonitis, representing a contained intra-abdominal infection. The patient’s diagnosis was particularly challenging due to the coexistence of advanced cardiovascular disease, recent coronary stenting, and ongoing DAPT, which markedly increased the risk of perioperative complications, including hemodynamic instability, myocardial ischemia, and bleeding. This combination of surgical urgency and high cardiac risk underscored the need for careful planning and expedited operative intervention.
Treatment
Although current guidelines generally recommend delaying noncardiac surgery for 3–6 months following drug-eluting stent implantation, our patient required urgent surgical intervention because of perforated appendicitis, making further postponement clinically unsafe. Delaying surgery would have exposed the patient to substantial risks related to ongoing intra-abdominal infection and sepsis.
Emergency laparoscopic appendicectomy was undertaken given the risk of progression to generalized peritonitis and sepsis. The patient was transferred to the operating theatre, where standard monitoring was applied. Invasive arterial blood pressure monitoring was established prior to induction of anesthesia (Fig. 3). Comprehensive monitoring in accordance with ASA guidelines was instituted, incorporating transesophageal echocardiography (TEE) to evaluate cardiac function and optimize fluid therapy (Figs. 4, 5). General anesthesia was delivered with comprehensive invasive hemodynamic monitoring and carefully titrated vasopressor support, allowing safe completion of the procedure and an uneventful postoperative recovery.
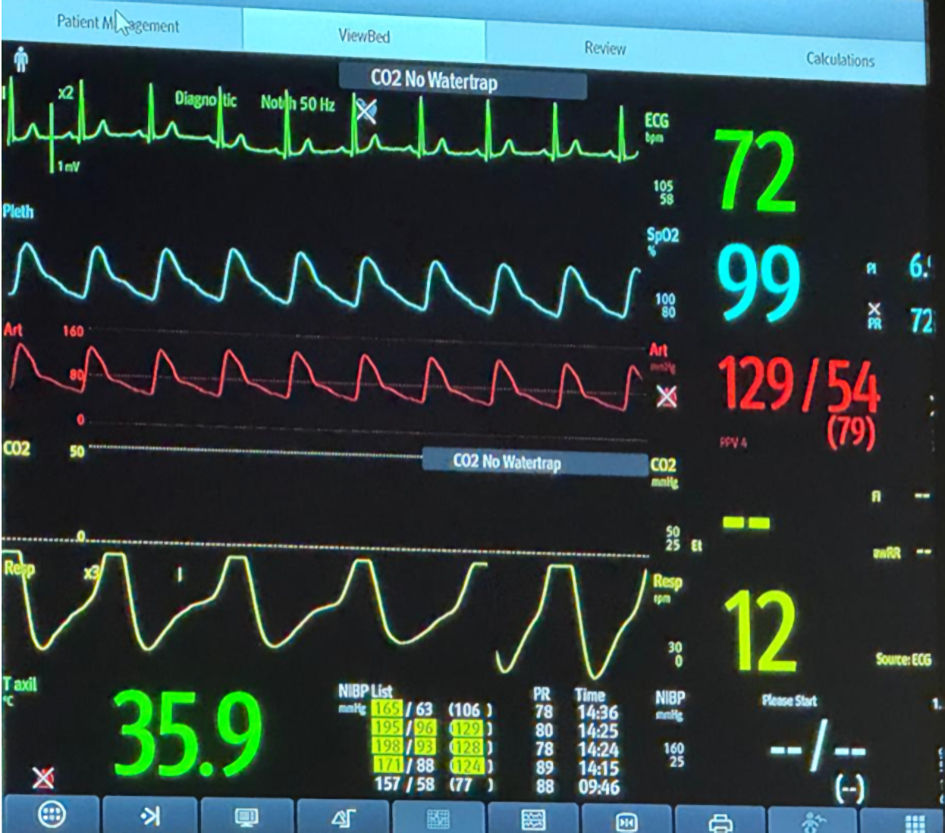 Click for large image | Figure 3. Hemodynamic intraoperative monitoring. |
 Click for large image | Figure 4. Intraoperative transesophageal echocardiography showing mitral regurgitation; color Doppler demonstrates systolic flow from the left ventricle to the left atrium (white arrow). |
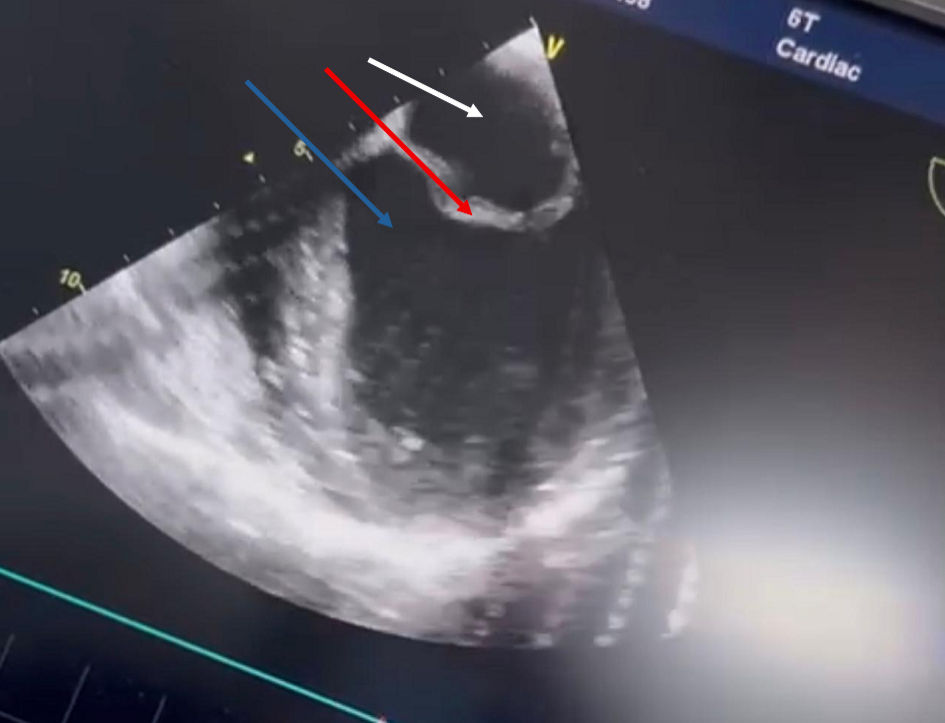 Click for large image | Figure 5. Intraoperative transesophageal echocardiography of the left atrium and ventricle for functional assessment and fluid guidance (left atrium: white arrow; mitral valve: red arrow; left ventricle: blue arrow). |
General anesthesia was induced and maintained with a remifentanil infusion and sevoflurane. A central venous catheter was inserted following induction to facilitate hemodynamic monitoring and administration of vasoactive agents.
Intraoperatively, hemodynamic support with a norepinephrine 0.05–0.1 µg/kg/min infusion was required to maintain adequate arterial pressure and coronary perfusion. The patient was mechanically ventilated using a lung-protective strategy (tidal volume 6 mL/kg, plateau pressure < 30 cm H2O, and driving pressure < 13 cm H2O), with a low level of positive end-expiratory pressure (5 cm H2O). A laparoscopic appendectomy was performed with the patient in approximately 30° Trendelenburg position, using a low pneumoperitoneum pressure (8–10 mm Hg) to minimize impairment of venous return, preload, and renal perfusion. Intraoperative findings revealed a retrocecal, perforated appendix. Careful dissection was undertaken, the appendix was removed, and the stump secured. Extensive peritoneal lavage was performed. The total operative time was approximately 3 h. Table 1 summarizes the main perioperative anesthetic and hemodynamic parameters, including anesthetic agents, intraoperative mean arterial pressure targets, blood loss estimation, perioperative hemoglobin trend, and postoperative cardiac evaluation.
 Click to view | Table 1. Perioperative Anesthetic, Hemodynamic, and Postoperative Cardiac Assessment Parameters |
Follow-up and outcomes
At the end of the procedure, the patient was carefully extubated and transferred to the intensive care unit for close monitoring. Hemodynamic parameters remained stable and drain output showed no evidence of postoperative bleeding. Although postoperative myocardial injury after noncardiac surgery (MINS) is an important perioperative consideration, postoperative troponin levels, electrocardiogram (ECG) evaluation, and transthoracic echocardiography examination in our patient showed no evidence of myocardial injury, and no changes on kinetics and ejection fraction compared to preoperative evaluation. DAPT with prasugrel and aspirin was continued throughout the perioperative period without interruption, and the first postoperative doses were administered on postoperative day 1. No anticoagulation was administered. Intravenous antibiotics were given for 5 days to treat peritonitis. The postoperative course was uneventful. The patient was discharged on the fifth postoperative day. Follow-up at 1 week was unremarkable, and he remained in good clinical condition at 1 month.
| Discussion | ▴Top |
CAD and coronary stents in the perioperative period: surgical timing and DAPT management
Emergency noncardiac surgery in patients with advanced CAD and recent coronary stent implantation poses a considerable clinical challenge, as it requires balancing the risks of perioperative bleeding with those of stent thrombosis. Interruption of DAPT is a well-established trigger for acute stent thrombosis, a complication associated with significant morbidity and mortality, particularly in patients with high-risk coronary anatomy, including left main disease, multivessel involvement, and impaired left ventricular function. Conversely, continuation of DAPT increases the risk of surgical bleeding, necessitating meticulous perioperative planning and mitigation strategies.
Current guidelines generally recommend delaying elective noncardiac surgery until after the critical post-stent period, at least 1 month for bare-metal stents and 3–6 months for drug-eluting stents [5–7]. However, these recommendations may be often impractical in urgent or emergent scenarios, underscoring the limitations of guideline-based approaches and highlighting the need for individualized decision-making.
Although current guidelines recommend delaying noncardiac surgery after drug-eluting stent implantation, several studies suggest that urgent surgery may be performed safely in carefully selected patients when delay is not feasible [8–10]. In our case, acute perforated appendicitis precluded postponement, requiring an individualized multidisciplinary strategy balancing thrombotic and bleeding risks.
Premature discontinuation of DAPT remains the strongest predictor of stent thrombosis, particularly within the first weeks to months after PCI, and is associated with high mortality [11–14]. Although our patient had not yet received the scheduled antiplatelet doses on the day of surgery, we deliberately chose to continue DAPT because of the extremely high thrombotic risk related to recent stenting and critical left main disease. This decision aligns with evidence suggesting that continuation of antiplatelet therapy may reduce ischemic complications without substantially increasing bleeding in urgent surgery [15–18].
To mitigate perioperative risk, a minimally invasive laparoscopic approach with low pneumoperitoneum pressures was selected, combined with comprehensive invasive hemodynamic monitoring and TEE, allowing continuous assessment of cardiovascular function throughout the procedure [19]. Table 2 [8–12, 14–23] summarizes the key findings of relevant studies and their relevance to our case. Our patient presented with acute perforated appendicitis, making surgical delay impossible. Management closely followed established perioperative principles for patients with coronary stents. Although discontinuation of DAPT was technically possible because the patient had not yet received the scheduled doses on the day of surgery, the decision was made to continue both agents perioperatively in view of the extremely high risk of catastrophic stent thrombosis. A minimally invasive laparoscopic approach was chosen to limit surgical stress and promote faster recovery, while low pneumoperitoneum pressures were used to minimize adverse effects on venous return, preload, and end-organ perfusion. Comprehensive invasive hemodynamic monitoring, complemented by TEE, enabled continuous assessment and optimization of blood pressure, heart rate, ventricular function, and tissue perfusion, ensuring strict cardiovascular stability throughout the perioperative period.
Click to view | Table 2. Summary of Key Studies on Perioperative Management After Coronary Stenting and Their Relevance to Our Case |
The decision to maintain DAPT was primarily guided by the patient’s very high thrombotic risk, including recent stent implantation and critical left main coronary stenosis, where the consequences of stent thrombosis were considered greater than the risk of surgical bleeding, as recent literature recommended [20, 21]. In addition, the laparoscopic approach helped mitigate hemorrhagic risk by reducing tissue trauma and intraoperative blood loss despite ongoing antiplatelet therapy.
Anesthetic considerations in perioperative management
Morgan et al [24] outline key anesthetic principles for ischemic heart disease patients undergoing noncardiac surgery, emphasizing maintenance of myocardial oxygen supply–demand balance. Management should avoid tachycardia, hypotension, and hypertension, which can precipitate ischemia. Both volatile agents and propofol-based techniques are acceptable, with emphasis on hemodynamic stability and stress response control. Individualized anesthetic plans, appropriate invasive monitoring, and meticulous fluid and vasopressor management are recommended. Continuation of beta-blockers and guideline-directed therapy, alongside adequate analgesia, is advised to minimize sympathetic activation [22–25].
Lung-protective ventilation strategies were applied throughout the procedure, including the use of low tidal volumes, plateau pressures below 30 cm H2O, and driving pressures below 13 cm H2O. This approach aimed to minimize ventilator-induced lung injury while maintaining adequate oxygenation and respiratory mechanics during laparoscopic surgery [26].
Multidisciplinary collaboration was central to the favorable outcome, enabling coordinated risk assessment and perioperative planning. Table 3 summarizes key anesthetic and preoperative concepts.
Click to view | Table 3. Key Anesthetic Recommendations for Patients With Coronary Stents Undergoing Noncardiac Surgery |
Intraoperative management in our case adhered to these principles, maintaining myocardial oxygen balance, avoiding hemodynamic swings, applying lung-protective ventilation, low pneumoperitoneum pressures, and comprehensive invasive monitoring. Real-time adjustments of anesthetic depth, fluids, and vasoactive agents allowed precise cardiovascular control and minimized myocardial stress, consistent with literature recommendations for high-risk cardiac patients [22–26].
Postoperative management and monitoring in high-risk cardiac patients
Postoperatively, vigilant surveillance for bleeding and cardiac complications was essential. Continuation of DAPT and close hemodynamic monitoring contributed to an uneventful recovery, though these results cannot be generalized.
Sellers et al emphasize that cardiovascular complications are major contributors to postoperative morbidity and mortality in patients with prior coronary stents, including MINS, myocardial infarction, arrhythmias, and heart failure. Many ischemic events are clinically silent, and stent thrombosis remains a rare but often fatal complication associated with premature DAPT discontinuation and the prothrombotic surgical milieu [27].
Postoperative care should be structured, clinically guided, and focused on cardiovascular risk reduction and early complication detection. Our patient, a 68-year-old man with severe multivessel CAD, critical left main stenosis, recent stenting, and ongoing DAPT, required careful attention to ischemic symptoms, ECG changes, and hemodynamic stability. Hypotension, tachycardia, anemia, and hypoxemia were actively avoided. Antiplatelet therapy was resumed as early as safely feasible, balancing bleeding and thrombotic risks. Follow-up prioritized clinical assessment, functional status, and risk factor management, with additional testing reserved for suspected ischemia. This approach underscores the importance of vigilant, symptom-guided monitoring and multidisciplinary coordination in optimizing postoperative outcomes.
Limitations
This report is limited by its single-case design, which restricts the generalizability of the findings and prevents definitive conclusions regarding optimal perioperative management in similar high-risk patients. Although current perioperative and cardiovascular guidelines are well established, individual patients often present unique clinical challenges requiring tailored multidisciplinary decision-making based on the balance between surgical urgency and cardiovascular risk. In our case, management decisions were individualized according to the patient’s urgent surgical indication and complex cardiovascular condition. Future studies involving larger cohorts are needed to better define perioperative anesthetic strategies, hemodynamic management, and optimal timing of urgent noncardiac surgery following recent drug-eluting stent implantation in patients with severe cardiac dysfunction.
Conclusions
This case illustrates the challenges of perioperative management in a patient with recent coronary stenting, severe multivessel CAD, impaired left ventricular function, and urgent perforated appendicitis requiring emergency surgery. While the management approach was based on established guideline-supported perioperative principles rather than a novel therapeutic strategy, the case highlights the importance of individualized multidisciplinary decision-making when balancing thrombotic, bleeding, and hemodynamic risks in situations where surgical delay is not feasible. The successful integration of continued DAPT, minimally invasive laparoscopic surgery, and advanced hemodynamic monitoring including TEE demonstrates the practical application of these principles in a particularly high-risk clinical setting.
Learning points
Urgent surgery in recently stented patients is high-risk: early intervention is sometimes unavoidable, but careful balancing of bleeding and thrombotic risk is critical.
Continuation of DAPT is generally protective: maintaining antiplatelet therapy, especially aspirin, reduces the risk of stent thrombosis, even if it may increase perioperative bleeding.
Minimally invasive approaches and low insufflation pressures: laparoscopic techniques with low pneumoperitoneum can limit hemodynamic compromise, reducing perioperative cardiovascular stress.
Physiology-guided anesthesia care: focus on maintaining myocardial oxygen supply–demand balance, avoiding tachycardia, hypotension, or abrupt hypertension, with lung-protective ventilation and careful fluid/vasopressor management.
Multidisciplinary planning and invasive monitoring: coordination among surgery, anesthesia, and cardiology teams, combined with continuous hemodynamic monitoring, enables individualized risk management and optimal perioperative outcomes.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Informed consent was obtained.
Author Contributions
BA and RD wrote the paper. AA, GH, VE, RK, AS and MV contributed to literature searching. AC, KL, MB, MN, FC, and EN contributed to language editing.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Rahgozar S, Elsayed N, Paraskevas KI, Han SM, Shalhub S, Malas MB. Factors associated with myocardial infarction among patients without prior history of coronary artery diseases following carotid artery revascularization. J Vasc Surg. 2026.
doi pubmed - Deeva ES, Isaikina MA, Trushina OI, Fomin VV, Pogonin AV, Tamkaeva MK. [Gastrointestinal complications of dual antiplatelet therapy in patients with ischemic heart disease: risk stratification, current management tactics. A review]. Ter Arkh. 2026;98(2):125-130.
doi pubmed - Battenberg A, Bell MR, Singh M, Jaffe AS, Tweet MS. Balancing bleeding and ischemic risk: dual antiplatelet therapy in a 90-year-old man with myocardial infarction and gastrointestinal bleeding. Am J Case Rep. 2026;27:e949920.
doi pubmed - Kiran U, Makhija N. Patient with recent coronary artery stent requiring major non cardiac surgery. Indian J Anaesth. 2009;53(5):582-591.
pubmed - Writing Committee Members, Thompson A, Fleischmann KE, Smilowitz NR, de Las Fuentes L, Mukherjee D, Aggarwal NR, et al. 2024 AHA/ACC/ACS/ASNC/HRS/SCA/SCCT/SCMR/SVM guideline for perioperative cardiovascular management for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2024;84(19):1869-1969.
doi pubmed - American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery), American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). Anesth Analg. 2008;106(3):685-712.
doi pubmed - Halvorsen S, Mehilli J, Cassese S, Hall TS, Abdelhamid M, Barbato E, De Hert S, et al. 2022 ESC Guidelines on cardiovascular assessment and management of patients undergoing non-cardiac surgery. Eur Heart J. 2022;43(39):3826-3924.
doi pubmed - Lee SH, Lee EK, Ahn HJ, Lee SM, Kim JA, Yang M, Choi JW, et al. Comparison of early and late surgeries after coronary stent implantation in patients with normal preoperative troponin level: a retrospective study. J Clin Med. 2023;12(7):2524.
doi pubmed - Xu Z, Lai Y, Zhou Y, Qin L, Hao X, Li T, Gao L, et al. The timing of surgical interventions following the implantation of coronary drug-eluting stents in patients undergoing gastrointestinal cancer surgery: a multicenter retrospective cohort study. Int J Surg. 2025;111(2):1724-1734.
doi pubmed - Choi CU, Rha SW, Jin Z, Chen KY, Minami Y, Kim JH, Na JO, et al. The optimal timing for non-cardiac surgery after percutaneous coronary intervention with drug-eluting stents. Int J Cardiol. 2010;139(3):313-316.
doi pubmed - Sharma AK, Ajani AE, Hamwi SM, Maniar P, Lakhani SV, Waksman R, Lindsay J. Major noncardiac surgery following coronary stenting: when is it safe to operate? Catheter Cardiovasc Interv. 2004;63(2):141-145.
doi pubmed - Gurajala I, Gopinath R. Perioperative management of patient with intracoronary stent presenting for noncardiac surgery. Ann Card Anaesth. 2016;19(1):122-131.
doi pubmed - Riddell JW, Chiche L, Plaud B, Hamon M. Coronary stents and noncardiac surgery. Circulation. 2007;116(16):e378-382.
doi pubmed - Yoon HK, Jun K, Park SK, Ji SH, Jang YE, Yoo S, Kim JT, et al. Anesthetic agents and cardiovascular outcomes of noncardiac surgery after coronary stent insertion. J Clin Med. 2020;9(2):429.
doi pubmed - Damazo-Escobedo CA, Vieyra-Herrera G, Martinez-Rios MA, Garcia-Navarrete MG, Silva-Ruz C. Coronary stent and prolonged dual antiplatelet therapy. A longitudinal study. Gac Med Mex. 2022;158(4):216-221.
doi pubmed - Vicenzi MN, Meislitzer T, Heitzinger B, Halaj M, Fleisher LA, Metzler H. Coronary artery stenting and non-cardiac surgery—a prospective outcome study. Br J Anaesth. 2006;96(6):686-693.
doi pubmed - Faloye A, Choudhury N, Gupta RG. Perioperative aspirin management in stable patients with coronary stents undergoing noncardiac surgery: hold or continue? J Cardiothorac Vasc Anesth. 2025;39(5):1113-1115.
doi pubmed - Rohatgi N, Zehnder JL, Smilowitz NR. Management of antiplatelet therapy in patients with coronary stents undergoing noncardiac surgery. Am J Med. 2022;135(9):e305-e307.
doi pubmed - Brilakis ES, Banerjee S, Berger PB. Perioperative management of patients with coronary stents. J Am Coll Cardiol. 2007;49(22):2145-2150.
doi pubmed - Rossini R, Tarantini G, Musumeci G, Masiero G, Barbato E, Calabro P, Capodanno D, et al. A multidisciplinary approach on the perioperative antithrombotic management of patients with coronary stents undergoing surgery: surgery after stenting 2. JACC Cardiovasc Interv. 2018;11(5):417-434.
doi pubmed - van Kuijk JP, Flu WJ, Schouten O, Hoeks SE, Schenkeveld L, de Jaegere PP, Bax JJ, et al. Timing of noncardiac surgery after coronary artery stenting with bare metal or drug-eluting stents. Am J Cardiol. 2009;104(9):1229-1234.
doi pubmed - Barash P, Akhtar S. Coronary stents: factors contributing to perioperative major adverse cardiovascular events. Br J Anaesth. 2010;105(Suppl 1):i3-15.
doi pubmed - Watkin D, Montgomery H, Gilbert-Kawai N. Cardiovascular assessment for non-cardiac surgery: updated European guidelines. Br J Hosp Med (Lond). 2023;84(9):1-8.
doi pubmed - Morgan H, Ezad SM, Rahman H, De Silva K, Partridge JSL, Perera D. Assessment and management of ischaemic heart disease in non-cardiac surgery. Heart Int. 2023;17(2):19-26.
doi pubmed - Hanci V, Yurtlu BS, Domi R, Shibata Y, Eyigor C. Acute postoperative pain control. Pain Res Manag. 2017;2017:7831014.
doi pubmed - Writing Committee; Steering Committee; PROTHOR Collaborative Group; PROtective VEntilation Network (PROVE Network) for the Clinical Trial Network of the European Society of Anaesthesiology and Intensive Care. Effects of intraoperative higher versus lower positive end-expiratory pressure during one-lung ventilation for thoracic surgery on postoperative pulmonary complications (PROTHOR): a multicentre, international, randomised, controlled, phase 3 trial. Lancet Respir Med. 2026;14(1):17-28.
doi pubmed - Sellers D, Srinivas C, Djaiani G. Cardiovascular complications after non-cardiac surgery. Anaesthesia. 2018;73(Suppl 1):34-42.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.