| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://jmc.elmerpub.com |
Case Report
Volume 16, Number 12, December 2025, pages 467-474

Radial Extracorporeal Shockwave Therapy for the Treatment of Chronic Refractory Coccygodynia
Michele Venosaa, b, Andrea Vespasianic, e ![]() , Emilio
Romaninia, b, Monica Nigric, Andrea Fidanzac, Giandomenico
Logroscinoc, d
, Emilio
Romaninia, b, Monica Nigric, Andrea Fidanzac, Giandomenico
Logroscinoc, d
aRomaPro Center for Hip and Knee Arthroplasty - Polo Sanitario San Feliciano, Rome
00166, Italy
bGLOBE, Italian Working Group on Evidence Based Orthopaedics, Rome
00197, Italy
cDepartment of Life, Health and Environmental Sciences, University
of L’Aquila, L’Aquila 67100, Italy
dDepartment of Mini-Invasive
and Computer-Assisting Orthopaedic Surgery, San Salvatore Hospital, L’Aquila 67100,
Italy
eCorresponding Author: Andrea Vespasiani, Department of Life, Health and
Environmental Sciences, University of L’Aquila, L’Aquila 67100, Italy
Manuscript submitted July 3, 2025, accepted August 8, 2025, published online November 22,
2025
Short title: ESWT for Refractory Coccygodynia
doi:
https://doi.org/10.14740/jmc5161
| Abstract | ▴Top |
Coccygodynia, characterized by persistent pain in the coccyx area, is a debilitating condition with limited effective treatments. We report a case exploring the use of radial extracorporeal shockwave therapy (ESWT) as a noninvasive treatment for chronic refractory coccygodynia. A 39-year-old female patient presented with chronic coccygeal pain unresponsive to conventional therapies. A thorough review of the patient’s medical history, clinical presentation, and imaging findings led to a diagnosis of idiopathic coccygodynia. Given her clinical situation and the failure of previous interventions, radial ESWT was considered a possible option due to its noninvasive nature and reported success in treating other chronic musculoskeletal conditions. Significant pain reduction and improved quality of life were observed 3 months post-treatment, as confirmed by the Visual Analog Scale (VAS), Pain Self Efficacy Questionnaire, Oswestry Disability Index, and Tampa Scale of Kinesiophobia scores. The beneficial effects were confirmed even at 12 months post-treatment follow-up, suggesting radial ESWT is a promising alternative therapeutic option. The positive outcomes in this case (though the evident limits of a case report) provide a foundation for considering radial ESWT in the broader context of managing chronic treatment-resistant coccygeal pain.
Keywords: Coccygeal region; Caudal vertebrae; Extracorporeal shockwave therapy; Chronic primary pain
| Introduction | ▴Top |
Coccygodynia, also known as coccydynia or tailbone pain, is a condition characterized by persistent pain at the coccyx, the terminal portion of the vertebral column. This condition can significantly impact a patient’s quality of life, affecting his/her ability to perform daily activities and diminishing overall well-being [1]. The pain associated with coccygodynia is often exacerbated by sitting, transitioning from sitting to standing, and during bowel movements. In severe cases, the pain can be debilitating, leading to chronic disability and psychological distress. It is a relatively common condition, but the exact prevalence rate is not well known [2]. Factors related to the high risk of developing coccydynia are female sex and obesity, as body mass index (BMI) may affect how a person sits or the amount of weight placed upon the coccyx [3]. Coccygodynia is five times more common in females than in males; the higher incidence in women is often attributed to anatomical differences, such as a broader pelvis and greater posterior tilt of the coccyx, as well as trauma related to childbirth [2]. The etiology of coccygodynia can be multifactorial. Common causes include trauma (such as falls or direct blows to the tailbone), repetitive strain or prolonged sitting on hard surfaces, degenerative changes in the coccygeal joint, and childbirth-related injuries [4]. Less commonly, coccygodynia can be secondary to local infections, tumors, or referred pain from lumbar spine pathologies. In some cases, coccygodynia can be idiopathic, with no identifiable cause [3]. The pathophysiology of coccygodynia involves inflammation, mechanical instability, or hypermobility of the coccyx. Inflammatory responses may occur due to local trauma or repetitive stress; hypermobility or instability of the coccyx can result from ligamentous laxity or joint degeneration, causing abnormal movement and subsequent pain. Additionally, changes in the surrounding musculature, such as the pelvic floor muscles, can contribute to coccygeal pain through altered biomechanics and muscle tension [5]. The management of coccygodynia typically begins with conservative approaches, but this condition is often unresponsive, and a gold standard is still lacking [6]. Radial extracorporeal shockwave therapy (ESWT) might be considered a possible option due to its reported success in treating other chronic musculoskeletal conditions [7]. Only a few studies have investigated the role of ESWT in the management of coccygodynia, but there is no standardized protocol in terms of shots and doses and none of them have assessed the psychological implications.
Given this background, we report a case of chronic refractory coccygodynia presenting a detailed account of radial ESWT in the conservative management of this pathology. By documenting the patient’s clinical presentation, treatment course, and outcomes (in terms of pain, function, and psychological impact), this report seeks to provide insights into the potential benefits and limitations of radial ESWT for managing coccygeal pain.
| Case Report | ▴Top |
A 39-year-old female (with a BMI of 20.7) presented with a 2-year history of severe coccygeal pain. The pain, described as sharp, persistent, and sometimes throbbing, was significantly aggravated by activities such as sitting or standing from a seated position. The pain intensity was assessed with the Visual Analog Scale (VAS) reporting a score of 7/10 and with the Pain Self Efficacy Questionnaire (PSEQ) reporting a score of 11 (range 0 - 60, higher scores indicate greater self-efficacy). The patient reported a significant impact on her quality of life, including difficulty performing daily activities, decreased mobility, and emotional distress due to chronic pain. The pain affected her ability to perform her job, which required prolonged periods of sitting, leading to frequent absenteeism and reduced productivity. Socially, she experienced difficulty participating in family activities and recreational pursuits, leading to feelings of isolation and frustration. The chronic nature of her pain also contributed to disturbed sleep patterns, resulting in fatigue and decreased overall well-being. The Oswestry Disability Index (ODI) score was 30/50 (moderate disability) and the Tampa Scale of Kinesiophobia (TSK) was 46 (range 0 - 52). In both these rating scales, a higher score reflects a worse outcome. Further inquiry into the patient’s history revealed no prior trauma to the coccygeal region, no recent childbirth, and no significant changes in weight that could have contributed to her condition. Previous interventions included multiple courses of nonsteroidal anti-inflammatory drugs (NSAIDs), which provided minimal pain relief and caused gastrointestinal discomfort. Physical therapy had focused on pelvic floor strengthening, but the benefits were short-lived, with pain returning shortly after each session. The patient’s overall health was otherwise unremarkable, with no chronic illnesses or other significant medical conditions. She had no previous history of psychological disorders, although the persistent pain had led to symptoms of anxiety and mild depression, for which she was not on medication. Her personal and family medical histories were also non-contributory to her current condition. The Depression Anxiety Stress Scale-21 (DASS-21) was administered at this phase to assess the psychological impact of this persistent clinical condition (depression score: 9 - moderate level; anxiety score: 5 - mild level; stress score: 10 - moderate level).
Physical examination revealed localized tenderness over the coccyx, with no palpable masses or visible deformities. The patient exhibited pain upon palpation of the sacrococcygeal junction and discomfort during rectal examination, which further localized the pain to the coccygeal area. Neurological examination was unremarkable, with no signs of radiculopathy or neurological deficits. The patient’s gait and posture were also assessed, revealing a tendency to avoid direct pressure on the coccyx by leaning forward while sitting and shifting weight frequently.
Imaging studies included pelvic radiographs and a magnetic resonance imaging (MRI) of the sacrococcygeal segment to rule out other potential causes of pain, such as tumors, infections, or significant degenerative changes. Anteroposterior and Maigne’s lateral dynamic X-rays of the lumbar spine and coccyx were performed to evaluate coccyx alignment; these excluded any dislocation or dynamic instability [8, 9]. MRI revealed no significant abnormalities that could account for the severity of the symptoms (Fig. 1). A thorough review of the patient’s medical history, clinical presentation, and imaging findings led to a diagnosis of idiopathic coccygodynia.
 Click for large image |
Figure 1. Sagittal MRI sacrococcygeal spine of the 39-year-old female patient affected by coccygodynia showing dehydrated L5S1 disc (withe arrow) with minimal posterior bulge (white dotted line arrow). No abnormalities were found on the tail bone (red arrow). On clinical examination, no lumbar pain or functional limitation of the lumbosacral spine was reported. MRI: magnetic resonance imaging. |
The lack of response to conventional treatments indicated a need for alternative therapeutic approaches. The patient was selected for radial ESWT after extensive discussions about the potential benefits, risks, and the current lack of effective relief from previous conventional treatments. Given her chronic, idiopathic coccygodynia and the failure of previous interventions, radial ESWT was considered a possible option due to its noninvasive nature and reported success in the management of coccygodynia itself [10], and other chronic musculoskeletal conditions such as plantar fasciopathy and lateral elbow epicondylopathy [7]. We decided to perform radial ESWT considering this approach is less invasive than other alternative procedures (ganglion impair block, local injections, radiofrequency ablation (RFA), coccygectomy).
After discussing various treatment options, including the potential benefits and risks, the patient consented to a therapeutic approach with radial ESWT. The procedure was conducted by a physiotherapist (with 15 years of experience) using a radial shockwave device specifically designed for musculoskeletal applications (Zimmer EnPuls 2.0 - Zimmer MedizinSysteme GmbH, Neu-Ulm, Germany). The patient was positioned comfortably on a treatment table to allow optimal access to the coccygeal region. A coupling gel was applied to facilitate the transmission of shockwaves through the skin and into the underlying tissues.
Treatment parameters included a frequency of 5 Hz and an energy flux density of 1 bar. Each session involved the delivery of 2,500 shocks, with adjustments based on patient feedback and tolerance, and treatments were administered once weekly for 5 weeks. These parameters were set based on the experience of our authors with previous cases of coccygodynia and mirror those utilized in similar radial ESWT research [11, 12]. The patient was monitored for adverse effects such as bruising, swelling, or increased pain, and was encouraged to maintain a pain diary to track symptoms and response to therapy. No significant adverse effects were reported.
Following each ESWT session, the patient was advised to avoid strenuous activities and prolonged sitting for the remainder of the day to prevent exacerbation of symptoms. Gentle stretching and mobility exercises were recommended to maintain flexibility and promote circulation in the coccygeal region (Table 1). The patient was also encouraged to use a cushioned seating pad to alleviate pressure on the coccyx during daily activities.
 Click to view |
Table 1. Stretching and Mobility Exercises for
Maintaining Flexibility and Promoting Circulation in the Coccygeal Region
Scheduled for the Patient |
Pain levels were assessed using the VAS and PSEQ, functional disability levels using the ODI questionnaire, and the patient’s fear of movement of re(injury) using the TSK before the first session and during follow-up visits at 3, 6, and 12 months post-treatment. The DASS-21 questionnaire was administered at each follow-up to assess the psychological implications of this condition. After completing the five ESWT sessions, the patient reported a significant reduction in pain.
At the 3-month follow-up, the patient showed significant improvement in all clinical scores, indicating sustained pain relief achieved after the ESWT. She reported being able to do daily activities that had previously been challenging, such as sitting comfortably for long periods, which was particularly beneficial for her office-based job. She also noted a decrease in the frequency and severity of pain flare-ups, which had previously been triggered by prolonged sitting or sudden movements. The patient reported better quality of life and better sleep, formerly disrupted by chronic pain. She was able to sleep through the night without waking due to discomfort, contributing to better overall health and daily functioning. Functionally, the patient demonstrated improved mobility and a greater range of motion in her lower back and pelvic region. Physical examinations at this stage showed reduced tenderness over the coccygeal area.
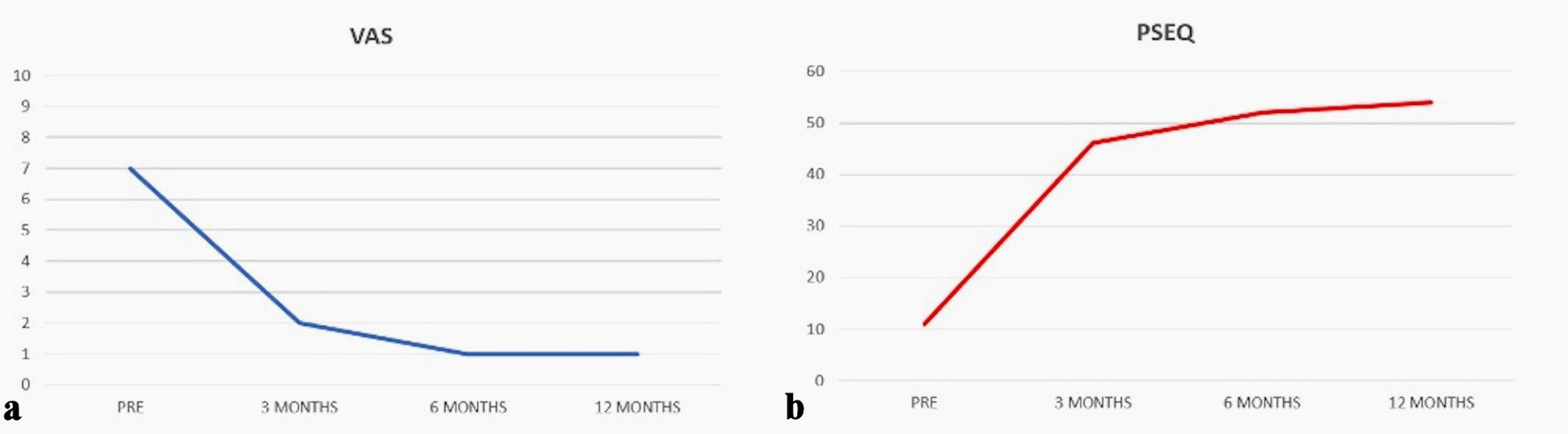
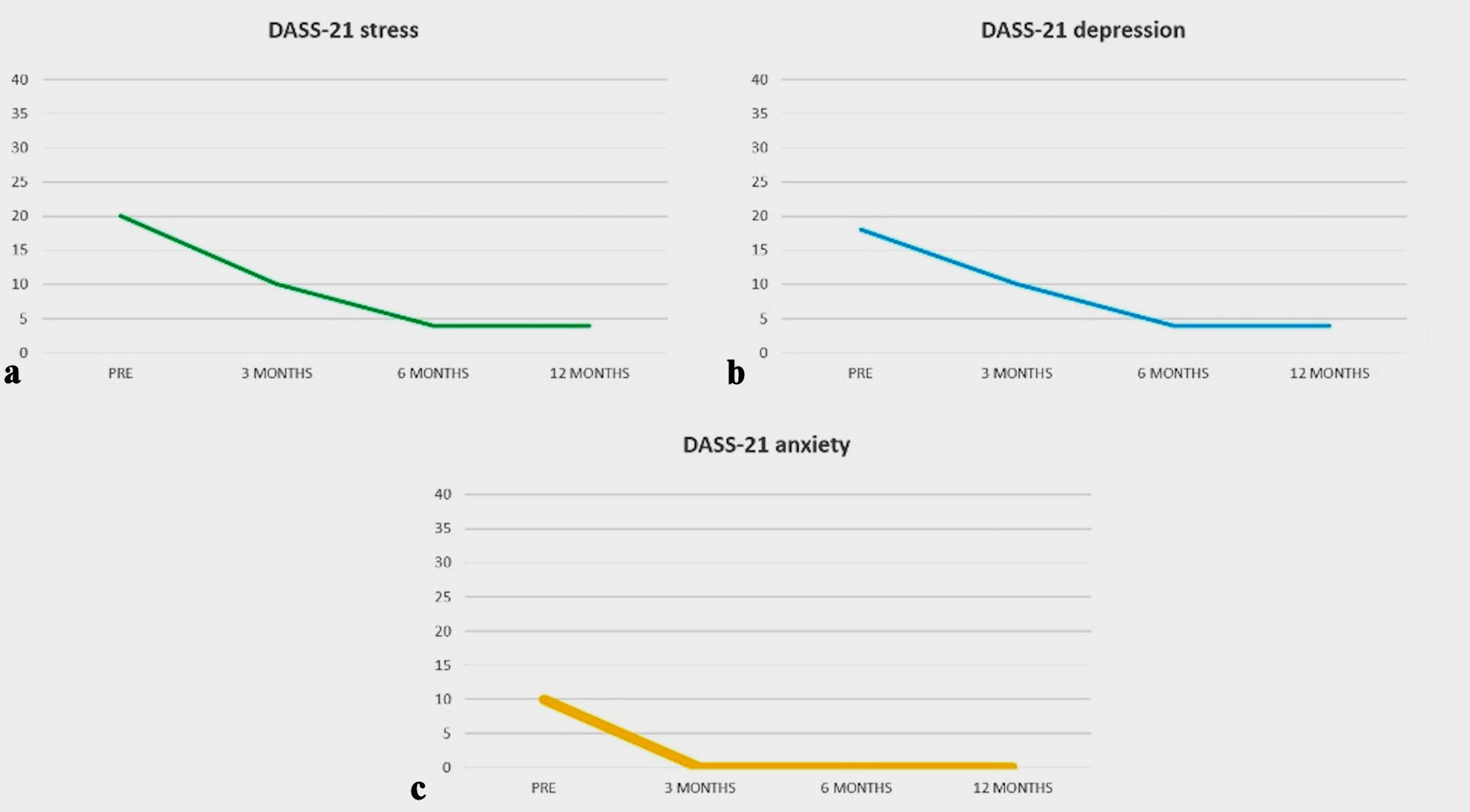
At the 12-month follow-up, the patient continued to experience sustained pain relief. Her VAS score reduced to 1/10, her ODI score reduced to 1/50 (no disability), PSEQ and TSK scores improved respectively to 54 and 26, and she reported a high level of satisfaction with the treatment outcomes. The patient resumed normal social activities and hobbies that she had previously abandoned. Her emotional well-being significantly improved, with reduced anxiety and depression symptoms related to chronic pain. These clinical results on the psychological side were confirmed by the progressive evolution of the DASS-21 score to normal levels at 12 months (depression score: 2; anxiety score: 0; stress score: 2). All data are reported in detail in Figures 2-4.
 Click for large image |
Figure 2. Changes in the pain perception measured with VAS (a) and PSEQ (b). The reduction in pain was already evident at 3 months and continued to improve until the last follow-up. VAS: Visual Analogue Scale; PSEQ: Pain Self Efficacy Questionnaire. |
 Click for large image |
Figure 3. Trends over time of the ODI (a) and TSK (b). Each score shows improved results over time. ODI: Oswestry Disability Index; TSK: Tampa Scale of Kinesiophobia. |
 Click for large image |
Figure 4. Trends over time of the DASS-21: stress score (a), depression score (b) and anxiety score (c). The charts show an improvement from a psychological perspective as well, with a reduction to normal levels of anxiety and stress at the 3-month follow-up, and to normal levels in each sub-scale at the final follow-up. DASS-21: Depression Anxiety Stress Scale-21. |
Additionally, the patient reported no adverse effects from the ESWT sessions. The absence of side effects contributed to her positive perception of the therapy and willingness to recommend it to others with similar conditions. The improvements in pain and functionality translated into significant enhancements in the patient’s overall quality of life. She reported greater productivity at work, fewer days off due to pain, and increased engagement in both professional and personal activities. The reduction in pain-related disability allowed her to perform daily tasks with ease and confidence, fostering a sense of normalcy that had been disrupted by her chronic condition. Emotionally, the patient experienced a reduction in stress and an improvement in mood. The alleviation of chronic pain played a crucial role in decreasing her anxiety and depressive symptoms, which were secondary to the persistent discomfort. The positive changes in her emotional state were corroborated by her family members, who noted her increased participation in family activities and social interactions. The patient expressed gratitude for the significant improvement in her condition, which had been unresponsive to previous treatments. She noted that the pain relief and functional gains achieved with radial ESWT far exceeded her expectations, given her long history of refractory coccygodynia.
| Discussion | ▴Top |
This study reports the efficacy of radial ESWT for treating chronic idiopathic coccygodynia, revealing significant reductions in pain and improvements in functional outcomes for a patient unresponsive to other conventional treatments. The rigorous monitoring of outcomes through standardized measures to assess pain, functional disability and limitations, and fear of movement due to chronic pain provided a reliable and structured evaluation of the treatment’s effectiveness over time. Furthermore, by documenting not just the physical outcomes but also the psychological impacts of chronic pain, the study offered a holistic view of patient health, addressing both the physical and emotional dimensions of pain. This could be considered one of the key points of this case report.
The management of coccygodynia typically begins with conservative approaches [5]. First-line treatments include the use of NSAIDs to reduce inflammation and alleviate pain. Alternatively, simple analgesics such as acetaminophen can provide pain relief, but their effectiveness varies among individuals. Other noninvasive interventions include the use of cushioned seating pads to relieve pressure on the coccyx and lifestyle modifications to avoid prolonged sitting. Using specially designed cushions to alleviate pressure on the coccyx while sitting can provide significant relief. Ergonomic adjustments in seating arrangements are also recommended. A study by Li et al showed the effects of the seat cushion contour and the sitting posture on surface pressure distribution and comfort during seated work. They found that proper contour design can improve pressure distribution during seating and increase the perception of comfort, thus contributing to pain reduction [13]. Physical therapy focusing on pelvic floor rehabilitation, postural adjustments, and core strengthening exercises can help improve function and reduce discomfort. Scott et al reported significant pain reduction in patients undergoing pelvic floor rehabilitation, highlighting its role in managing coccygodynia associated with pelvic floor dysfunction [14]. Seker et al and Nourani et al found that manual manipulation and mobilization techniques targeting the sacrococcygeal joint can provide pain relief for some patients [15, 16]. For patients who do not respond adequately to conservative measures, more invasive treatments may be considered. These include local corticosteroid injections to reduce inflammation and provide temporary pain relief, nerve blocks, and, in refractory cases, coccygectomy (surgical removal of the coccyx) [17]. However, these invasive procedures carry risks and may not provide long-term relief. Local injections, including corticosteroids and local anesthetics, are commonly used to provide temporary relief from pain. Finsen et al reviewed the efficacy of corticosteroid injections, finding that their effect on coccygodynia is moderate, possibly because of the use of modest doses of the drugs. Even so, they seem worthwhile as they are easily and quickly performed, with rare complications. They concluded that if the choice is between injections of betamethasone or triamcinolone, the latter should be selected [18]. An alternative procedure to corticosteroid injections involves injecting a local anesthetic and/or steroid into the ganglion impar. Nasiri et al reported significant pain reduction in patients receiving this treatment [19]. RFA involves the use of heat generated by radio waves to ablate the nerves transmitting pain signals from the coccyx. A study by Chen et al demonstrated that RFA could provide long-term pain relief for patients with chronic coccygodynia, with minimal side effects [20]. Surgical removal of the coccyx (coccygectomy) is considered a last resort for patients with intractable pain unresponsive to conservative and interventional treatments. In a study performed by Perna et al, the authors retrospectively examined 21 patients treated with coccygectomy showing significant improvements in disability and quality of life measures, with minimal complications, with only one case of superficial wound infection [21]. Given the limitations of conventional treatments, there is a growing interest in exploring alternative therapeutic options for coccygodynia. One such emerging therapy is ESWT. This case report demonstrates the potential efficacy of radial ESWT in treating chronic coccygodynia, a condition that is often difficult to manage with conventional therapies. The mechanisms by which ESWT may alleviate pain include mechanical disruption of pain pathways, increased local blood flow, and stimulation of tissue regeneration processes. Several hypotheses have been proposed based on current understanding, assuming mechanical, biological, neurological, and anti-inflammatory effects. The shockwaves generated during ESWT can produce microtrauma in the targeted tissues, leading to cellular responses that promote tissue repair and regeneration. This mechanical stimulation can disrupt pain signaling pathways and reduce pain perception. Moreover, ESWT has been shown to increase the expression of growth factors such as vascular endothelial growth factor (VEGF) and transforming growth factor-beta (TGF-β), which play crucial roles in angiogenesis and tissue healing. Enhanced blood flow and nutrient delivery to the affected area can accelerate the healing process and reduce inflammation. ESWT may modulate the activity of nociceptors and reduce the transmission of pain signals to the central nervous system. This neuromodulation effect can result in decreased pain sensitivity and improved pain tolerance. Lastly, ESWT has been reported to reduce levels of pro-inflammatory cytokines and increase the production of anti-inflammatory mediators. This shift in the inflammatory milieu can contribute to pain relief and improved tissue health [22]. These combined peripheral and central effects can help “desensitize” the nervous system, making it particularly relevant in idiopathic chronic musculoskeletal pain driven by central sensitization rather than overt tissue damage.
While ESWT has been extensively studied for conditions such as plantar fasciitis and lateral epicondylitis, its use in coccygodynia remains relatively unexplored. In the context of coccygodynia, a few case reports and small-scale studies have indicated positive outcomes with ESWT. For instance, in a study by Sah et al, both patients treated with focused ESWT and those treated with radial ESWT showed significant improvements in pain and function compared with baseline measurements. According to the results of their study, radial ESWT would appear to be more effective in the treatment of coccydynia [23]. A prospective study on 14 patients performed by Lota et al similarly affirms the safety and efficacy of radial ESWT in managing coccydynia. The treatment alleviated pain in all patients; no recurrence of symptoms was reported during follow-up with a positive correlation between symptom duration and the number of treatment sessions [10]. Ahadi et al prospectively compared the efficacies of ESWT and corticosteroid injections (34 patients randomized into two groups). In the ESWT group, patients received radial shockwave for three weekly sessions. The other group received an injection of steroid in the tip of the coccyx or sacrococcygeal junction. The VAS score was significantly decreased in all follow-ups in both groups. According to the results of this study, ESWT has proved to be an effective intervention in patients with coccydynia with more long-lasting efficacy than steroid injections in terms of pain relief over 6 months of observation [11].
The findings of these studies align with the outcomes observed in the present case, where the patient experienced substantial pain reduction and enhanced quality of life following ESWT. This growing body of evidence supports the hypothesis that ESWT may be a viable alternative for managing refractory coccygodynia.
This case report is inherently limited by its single-subject design. As a case report, it lacks the statistical power and generalizability that larger studies provide. The findings, while promising, cannot be extrapolated to a broader population without further investigation. The absence of a control group also means that it is difficult to attribute the observed improvements solely to ESWT; other factors such as placebo effects or spontaneous recovery could have contributed to the patient’s progress. Another limitation is the relatively short follow-up period. While the patient reported significant pain relief and functional improvement up to 12 months post-treatment, the long-term sustainability of these benefits remains unknown. Chronic pain conditions like coccygodynia often have fluctuating courses, and longer-term follow-up is necessary to determine if ESWT can provide lasting relief or if repeated treatments are required. The subjective nature of pain assessment is another potential limitation. The use of the VAS provides a measure of pain intensity, but it is inherently subjective and can be influenced by various factors including the patient’s psychological state and expectations. Anyway, the use of a standardized measure of functional evolution, such as the ODI index, has provided further confirmation of the therapeutic effects of ESWT.
To build on the findings of this case report, future research should focus on conducting randomized controlled trials (RCTs) with larger sample sizes. Future research should also explore the optimal treatment parameters for ESWT, including the frequency, intensity, and number of sessions required to achieve maximal therapeutic benefit. Comparative studies evaluating different ESWT protocols can help identify the most effective treatment regimens. Research should also explore the cost-effectiveness of ESWT compared with other treatment options for coccygodynia. Economic evaluations can help determine the value of ESWT in the healthcare system and inform clinical decision-making and policy development. Lastly, studies investigating potential predictors of response to ESWT, such as demographic factors, pain characteristics, and baseline functional status, would be valuable. Identifying which patients are most likely to benefit from ESWT can help tailor treatments to individual needs and improve overall treatment outcomes.
Learning points
This case report demonstrates that radial ESWT can be a promising noninvasive alternative in chronic refractory coccygodynia.
The report (although limited by its single-subject design) emphasizes the importance of a holistic approach, using standardized tools to measure physical disability, pain perception, fear of movement, and emotional distress
Acknowledgments
The manuscript has been prepared according to CARE guidelines for case reports.
Financial Disclosure
No funding was provided specifically for this project.
Conflict of Interest
Each author declares that he has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article.
Informed Consent
Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.
Author Contributions
Conception: MV; preparation of the manuscript: MV and MN; revision for important intellectual content: GL and AV; supervision: AF and ER. All authors read and approved the final manuscript.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Abbreviations
BMI: body mass index; DASS-21: Depression Anxiety Stress Scale-21; ESWT: extracorporeal shockwave therapy; MRI: magnetic resonance imaging; NSAIDs: nonsteroidal anti-inflammatory drugs; ODI: Oswestry Disability Index; PSEQ: Pain Self Efficacy Questionnaire; TSK: Tampa Scale of Kinesiophobia, VAS, Visual Analogue Scale
| References | ▴Top |
- Dampc B, Slowinski K. Coccygodynia - pathogenesis, diagnostics and
therapy. Review of the writing. Pol Przegl Chir. 2017;89(4):33-40.
doi pubmed - Lirette LS, Chaiban G, Tolba R, Eissa H. Coccydynia: an overview of
the anatomy, etiology, and treatment of coccyx pain. Ochsner J. 2014;14(1):84-87.
pubmed - Patijn J, Janssen M, Hayek S, Mekhail N, Van Zundert J, van Kleef M.
14. Coccygodynia. Pain Pract. 2010;10(6):554-559.
doi pubmed - Garg B, Ahuja K. Coccydynia-A comprehensive review on etiology,
radiological features and management options. J Clin Orthop Trauma.
2021;12(1):123-129.
doi pubmed - Daily D, Bridges J, Mo WB, Mo AZ, Massey PA, Zhang AS. Coccydynia: a
review of anatomy, causes, diagnosis, and treatment. JBJS Rev. 2024;12(5).
doi pubmed - Andersen GO, Milosevic S, Jensen MM, Andersen MO, Simony A, Rasmussen
MM, Carreon L. Coccydynia-the efficacy of available treatment options: a systematic review.
Global Spine J. 2022;12(7):1611-1623.
doi pubmed - Schroeder AN, Tenforde AS, Jelsing EJ. Extracorporeal shockwave
therapy in the management of sports medicine injuries. Curr Sports Med Rep.
2021;20(6):298-305.
doi pubmed - Maigne JY, Tamalet B. Standardized radiologic protocol for the study
of common coccygodynia and characteristics of the lesions observed in the sitting position.
Clinical elements differentiating luxation, hypermobility, and normal mobility. Spine (Phila Pa
1976). 1996;21(22):2588-2593.
doi pubmed - Maigne JY, Guedj S, Straus C. Idiopathic coccygodynia. Lateral
roentgenograms in the sitting position and coccygeal discography. Spine (Phila Pa 1976).
1994;19(8):930-934.
doi pubmed - Lota KS, Malliaropoulos N, Bikos G, Lohrer H. Radial extracorporeal
shockwave therapy (rESWT) for coccydynia: a prospective study of 14 patients. Ann Med Surg
(Lond). 2023;85(10):4656-4661.
doi pubmed - Ahadi T, Hosseinverdi S, Raissi G, Sajadi S, Forogh B. Comparison of
extracorporeal shockwave therapy and blind steroid injection in patients with coccydynia: a
randomized clinical trial. Am J Phys Med Rehabil. 2022;101(5):417-422.
doi pubmed - Gonen Aydin C, Orscelik A, Gok MC, Akman YE. The efficacy of
extracorporeal shock wave therapy for chronic coccydynia. Med Princ Pract.
2020;29(5):444-450.
doi pubmed - Li W, Mo R, Yu S, Chu J, Hu Y, Wang L. The effects of the seat
cushion contour and the sitting posture on surface pressure distribution and comfort during
seated work. Int J Occup Med Environ Health. 2020;33(5):675-689.
doi pubmed - Scott KM, Fisher LW, Bernstein IH, Bradley MH. The treatment of
chronic coccydynia and postcoccygectomy pain with pelvic floor physical therapy. PM R.
2017;9(4):367-376.
doi pubmed - Seker A, Sarikaya IA, Korkmaz O, Yalcin S, Malkoc M, Bulbul AM.
Management of persistent coccydynia with transrectal manipulation: results of a combined
procedure. Eur Spine J. 2018;27(5):1166-1171.
doi pubmed - Nourani B, Norton D, Kuchera W, Rabago D. Transrectal osteopathic
manipulation treatment for chronic coccydynia: feasibility, acceptability and patient-oriented
outcomes in a quality improvement project. J Osteopath Med. 2024;124(2):77-83.
doi pubmed - Elkhashab Y, Ng A. A review of current treatment options for
coccygodynia. Curr Pain Headache Rep. 2018;22(4):28.
doi pubmed - Finsen V, Kalstad AM, Knobloch RG. Corticosteroid injection for
coccydynia: a review of 241 patients. Bone Jt Open. 2020;1(11):709-714.
doi pubmed - Nasiri A, Farajzadeh Vajari F, Sane S, Afsargharehbagh R. Assessment
of ganglion impar block effect on treatment results of coccydynia: a cross-sectional study.
Anesth Pain Med. 2024;14(2):e142137.
doi pubmed - Chen Y, Huang-Lionnet JHY, Cohen SP. Radiofrequency ablation in
coccydynia: a case series and comprehensive, evidence-based review. Pain Med.
2017;18(6):1111-1130.
doi pubmed - Perna A, Franchini A, Macchiarola L, Maruccia F, Barletta F, Bosco F,
Rovere G, et al. Coccygectomy for refractory coccydynia, old-fashioned but effective procedure:
a retrospective analysis. Int Orthop. 2024;48(8):2251-2258.
doi pubmed - De la Corte-Rodriguez H, Roman-Belmonte JM, Rodriguez-Damiani BA,
Vazquez-Sasot A, Rodriguez-Merchan EC. Extracorporeal shock wave therapy for the treatment of
musculoskeletal pain: a narrative review. Healthcare (Basel). 2023;11(21):2830.
doi pubmed - Sah V, Elasan S, Kaplan S. Comparative effects of radial and focused
extracorporeal shock wave therapies in coccydynia. Turk J Phys Med Rehabil.
2023;69(1):97-104.
doi pubmed
This
article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0
International License, which permits unrestricted non-commercial use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Journal
of Medical Cases is published by Elmer Press Inc.