| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://jmc.elmerpub.com |
Case Report
Volume 16, Number 4, April 2025, pages 131-134

An Unusual Case of Pancreatic Adenocarcinoma Metastasis to the Trapezium Bone
Kyle S. Gordona, b, Talwinder Nagia, Raksha Sharmaa, Michael Mamonea, Stephane Buteaua, Warren Brennera
aDepartment of Internal Medicine, Boca Raton Regional Hospital, Florida Atlantic
University, Boca Raton, FL, USA
bCorresponding Author: Kyle S. Gordon,
Department of Internal Medicine, Boca Raton Regional Hospital, Florida Atlantic University, Boca
Raton, FL, USA
Manuscript submitted July 15, 2024, accepted April 1, 2025, published online April 16,
2025
Short title: Unusual Pancreatic Adenocarcinoma Metastasis
doi:
https://doi.org/10.14740/jmc4282
| Abstract | ▴Top |
Pancreatic adenocarcinoma is an aggressive malignancy that accounts for over 90% of pancreatic cancers. It is associated with a poor prognosis and a 5-year survival rate of less than 10%. In 2023, there were an estimated 64,050 new cases of pancreatic cancer and 50,550 related deaths. Common sites of metastasis include the liver, lungs, lymph nodes, and peritoneal cavity. While bone metastases can occur, metastatic disease involving the bones of the hand is exceedingly rare. In this report, we present a case of metastatic pancreatic cancer involving the trapezium bone of the hand, along with a review of the literature.
Keywords: Trapezium; Pancreatic adenocarcinoma; Distal bony metastasis
| Introduction | ▴Top |
Pancreatic adenocarcinoma constitutes 90% of pancreatic neoplasms and is an aggressive malignancy with few effective therapeutic options and a propensity for early metastasis [1]. Ranked as the fourth leading cause of cancer-related death in the United States [2, 3], early detection remains a formidable challenge, and the overall prognosis continues to be poor. Bone metastases in pancreatic adenocarcinoma are an uncommon occurrence, with a prevalence estimated to be between 10% and 20% [4, 5]. This case report describes the rarity of bone metastases to the hand, emphasizing the need for heightened vigilance in recognizing and managing unique presentations.
| Case Report | ▴Top |
An 80-year-old female was diagnosed with stage IV pancreatic adenocarcinoma with metastatic disease to the lungs and retroperitoneal lymph nodes. Subsequent re-imaging and biopsies conformed to malignant pancreatic adenocarcinoma. Genetic testing revealed both a somatic and germline ATM mutation. The patient initially received standard therapy with gemcitabine and nab paclitaxel, followed by disease progression. She subsequently received additional therapy with FOLFOX, followed by 5-fluorouracil (5-FU) and liposomal irinotecan. While receiving third-line chemotherapy, she presented with progressively worsening left wrist and thumb pain, accompanied by swelling and erythema over 3 months. The pain was primarily at the left thumb basal joint, was initially intermittent but progressed, and she denied any trauma to that location. Despite therapy for presumed pseudogout/inflammatory arthritis and nonspecific changes on X-rays, her pain became progressively worse, requiring hospitalization for pain control and additional investigation.
On admission, physical examination revealed a cachectic-appearing patient in significant discomfort. Evaluation of the left thumb carpometacarpal joint showed swelling with some erythema and decreased range of motion due to pain. Laboratory results were remarkable for an elevated erythrocyte sedimentation rate of 51 mm/h, C-reactive protein of 6.29 mg/dL (< 0.500 mg/dL is normal high), and alkaline phosphatase of 174 IU/L (normal low 35 and normal high 104).
Magnetic resonance imaging (MRI) of the left hand revealed findings of osteolysis suspicious for an underlying infiltrative process involving the entire trapezium bone and the base of the first metacarpal, associated with diffuse edema of the soft tissue, as depicted in Figure 1.
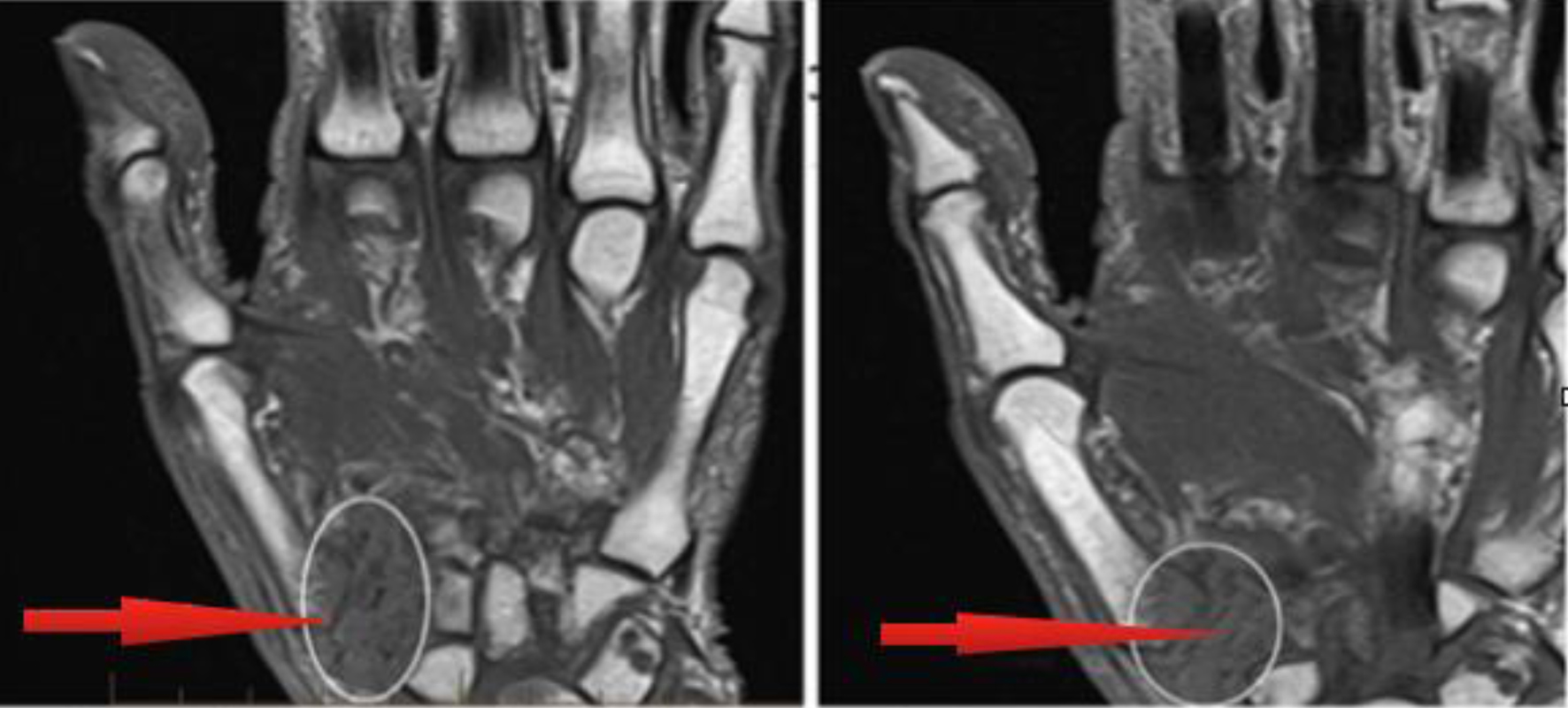 Click for large image |
Figure 1. Metastatic involvement of entire trapezium bone and base of first metacarpal associated with diffuse edema of soft tissue, with red arrows indicating metastatic involvement of pancreatic carcinoma. |
The patient was initiated on empiric vancomycin and ceftazidime due to initial concerns for septic arthritis with osteomyelitis. Orthopedic surgery was consulted and a surgical incision and drainage of the left thumb basilar joint and debridement was performed, revealing mucopurulent material, necrosis of the thumb metacarpal base, and evidence of significant erosion of the trapezium. Subsequently, an infectious workup, including blood cultures, pathology cultures/Gram stain, and fungal cultures, was unrevealing. Figure 2 depicts hematoxylin stain from surgical biopsy of left trapezium with red arrows depicting a nest of atypical cells supporting suspicion for malignant pancreatic carcinoma cells. Surgical pathology demonstrated in Figure 3 revealed necrotic bone with infiltration by metastatic moderately differentiated adenocarcinoma. Immunohistochemistry confirmed the neoplastic cells as pancytokeratin (+), cytokeratin (CK)7 (variably +), CK20 (-), CDX2 (-), and thyroid transcription factor 1 (TTF1) (-). CD68 highlighted abundant histiocytes. The overall findings aligned with metastatic pancreatic adenocarcinoma, correlating with the patient’s known history.
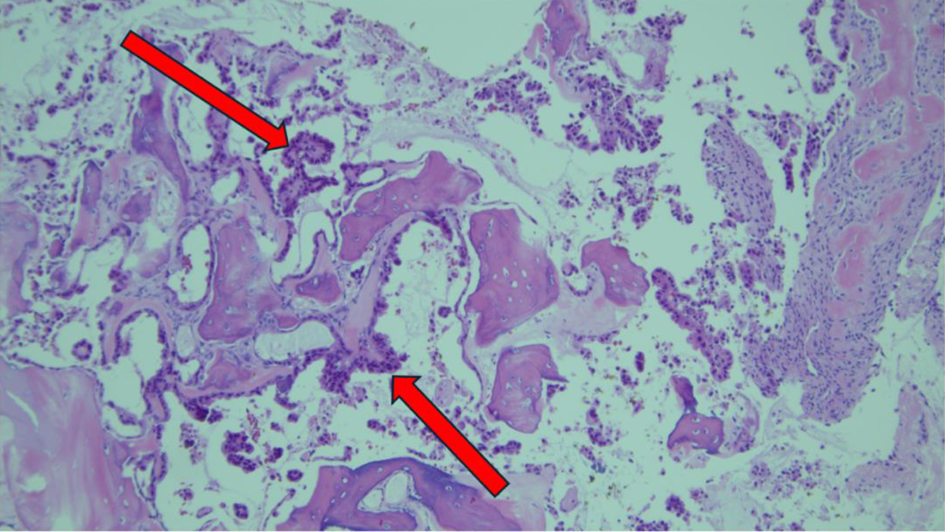
 Click for large image |
Figure 2. Hematoxylin stain from surgical biopsy of left trapezium with red arrow depicting a nest of atypical cells supporting suspicion for malignant pancreatic carcinoma cells. |
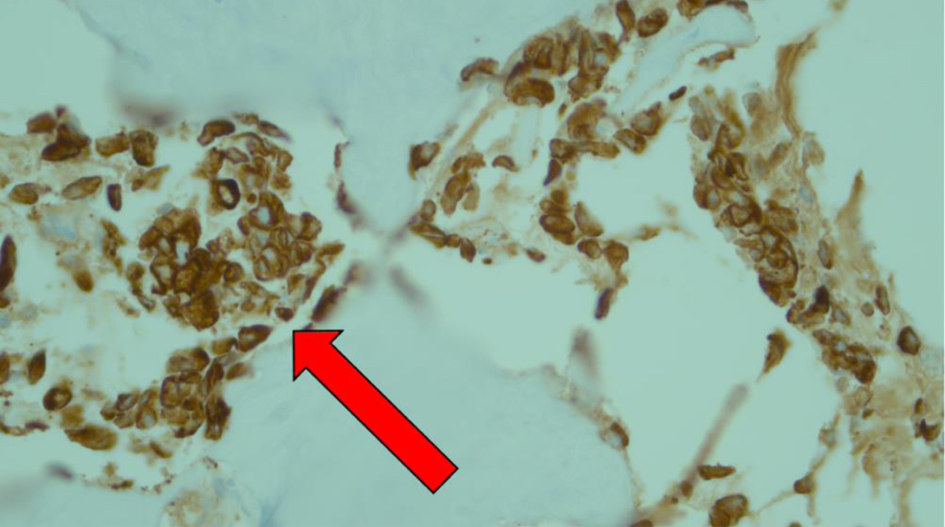
 Click for large image |
Figure 3. Immunohistochemistry staining from surgical biopsy of left trapezium. Red arrows depict strong cytoplasmic staining depicting neoplastic cells that are pancytokeratin (+), with CK7 (variably +), CK20 (-), CDX2 (-), and TTF1 (-). The neoplastic cells were noted with high expression of CD68, highlighting abundant histocytes. These findings were consistent with metastatic pancreatic adenocarcinoma. |
The patient was subsequently discharged and followed up as an outpatient with oncology for further consideration of palliative chemotherapy. However, given the poor prognosis and lack of additional therapeutic options, she elected to proceed with hospice care and passed away 6 weeks later.
| Discussion | ▴Top |
This unique case challenges conventional diagnostic expectations, emphasizing the need for heightened vigilance in atypical presentations. Our case is the first documented case of a distal extremity (trapezium) bone metastasis from pancreatic cancer.
The common metastatic locations from pancreatic cancer are the liver, lungs, and peritoneal cavity, with bone involvement being less common [6]. Both osteolytic and osteoblastic lesions from osseous pancreatic metastases have been described in the literature [6]. In a retrospective chart review study, 323 patients with pancreatic cancer were followed. The study found that seven out of 323 patients (2.2%) developed skeletal metastases during the course of their disease [6]. The most common sites of skeletal metastases were the vertebrae, hips, and ribs, while metastases to the upper and lower extremities and skull were far less common [6]. The time to development of skeletal metastases varied significantly, and patients with primary pancreatic cancer at the head of the pancreas had a higher risk for skeletal metastases. Conversely, an autopsy study found that 5-20% of patients with pancreatic cancer can have skeletal metastases, with a primary tumor in the tail being more likely to metastasize to the bone [7]. There was no documented involvement of any carpal bones during these studies, and the pathogenesis of osseous metastases remains poorly understood.
In general, cancer cells infiltrate and migrate to distant sites through the blood vessel walls to the extracellular space of the bone. Tumor cell adhesion is facilitated by E- and N-cadherin [8]. Bone involvement progresses when the physiologic remodeling process is disrupted by tumor cells through molecular mechanisms involving cytokines such as interleukin-6 (IL-6) and vascular endothelial growth factor (VEGF), as well as communication between osteoclasts, osteocytes, and osteoblasts [8].
In review of the online databases, from 2000 to 2024, we did not find any similar documented cases of pancreatic cancer with metastasis to the trapezium or any carpal bone. Two cases were identified that documented involvement of the humeral bone and the clavicle. One case involved a 77-year-old female presenting with severe tenderness in the right proximal humerus and reduced shoulder motion [9]. Further workup revealed elevated carbohydrate antigen (CA)-19 and carcinoembryonic antigen (CEA) levels, and X-ray imaging of the right humerus showed lytic lesions with metastatic features. A computed tomography (CT) scan of the abdomen and pelvis revealed a necrotic mass in the tail of the pancreas with metastases to the left adrenal gland and liver. A tissue sample from the right humerus confirmed metastatic adenosquamous carcinoma with mucoepidermoid morphology of pancreatic origin [9]. Most literature indicates that patients who develop osseous metastases already have concomitant visceral metastases.
Another case described a 46-year-old female with pancreatic adenocarcinoma who underwent a Whipple procedure and presented 2 years later with right clavicle pain [10]. CT imaging showed increased sclerosis of the medial right clavicular head with a moth-eaten appearance of the cortex and medullary space. A fine-needle biopsy confirmed metastatic pancreatic cancer. She was treated with zoledronic acid and completed a 2-week course of palliative radiation therapy to the affected clavicle. However, her course was complicated by newly developed pain in the left hip, with imaging revealing progression of metastatic bony disease and new lesions in the left sacrum. This case was unique in that no visceral metastases were identified.
Metastases to the trapezium have been documented in three cases involving malignancies other than pancreatic cancer. The first case involved a 62-year-old male with pain and massive swelling of the right carpometacarpal (CMC) joint of the thumb. Imaging revealed osteolytic lesions in the trapezium, with near-complete resorption. A needle biopsy confirmed adenocarcinoma [11]. A positron emission tomography (PET) scan and endoscopy revealed advanced gastric adenocarcinoma with no other distant metastases besides the trapezium. He underwent systemic chemoradiotherapy and eventual resection of the trapezium mass with hand reconstruction. Another case involved a 70-year-old male with a history of prostate cancer presenting with pain at the base of the right thumb. Imaging and biopsy revealed primary non-small cell lung carcinoma (NSCLC) with trapezium metastasis [12]. The final case described a female in her mid-40s with known NSCLC who presented with pain at the base of her right thumb, with imaging confirming trapezial involvement [13]. She underwent a trapezial excision with capsular interposition, and pathology confirmed metastatic NSCLC.
Conclusion
This case report illustrates a rare instance of pancreatic adenocarcinoma metastasis to the distal basilar thumb joint, highlighting the importance of maintaining a broad differential diagnosis in the management of patients with malignancies who present with atypical clinical findings. The insights gained contribute to the evolving understanding of atypical metastatic patterns, guiding future diagnostic and therapeutic approaches.
Learning points
We have the first known documented case of pancreatic cancer metastasizing to the trapezium, a distal carpal bone in the hand, expanding the known spectrum of osseous metastatic involvement.
Our unique case challenges conventional diagnostic expectations, which emphasizes the importance of maintaining a high index of suspicion for atypical presentations in pancreatic malignancy and other neoplastic presentations.
Pancreatic cancer most commonly metastasizes to the liver, lungs, and peritoneum; bone metastases are less common and typically involve the vertebrae, pelvis, and ribs. Involvement of the upper extremities or carpal bones is exceedingly rare.
Literature review revealed no prior cases of trapezium involvement by pancreatic cancer between 2000 and 2024. Two previously reported cases involved metastases to the humerus and clavicle, typically in the presence of visceral metastases.
Mechanisms of pancreatic bone metastasis involve tumor cell migration through vasculature, adhesion via cadherins, and disruption of normal bone remodeling through cytokines like IL-6 and VEGF.
Only three prior cases of trapezium metastasis from other primary cancers (gastric, prostate, and NSCLC) have been documented, underscoring the rarity of carpal bone involvement overall.
Our case reinforces the value of early imaging, biopsy, and consideration remaining cognizant of metastatic disease in patients with known malignancies presenting with unexplained musculoskeletal symptoms, even in atypical locations.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Not applicable.
Author Contributions
Kyle S. Gordon, MD: the corresponding author, composed the abstract, introduction, case description, and conclusion. Talwinder Nagi, MD: discussion, photo imagery. Stephane Buteau, MD: editorial support, attending internist on the case. Raksha Sharma, MD: MRI images, pathology slides, references. Michael Mamone, MD: attending internist on the case. Warren Brenner, MD: medical oncologist - Lynn Cancer Institute, editorial support.
Data Availability
Any inquiries regarding supporting data for this study should be directed to the corresponding author, Kyle S. Gordon, MD.
| References | ▴Top |
- Mao C, Domenico DR, Kim K, Hanson DJ, Howard JM.
Observations on the developmental patterns and the consequences of pancreatic exocrine
adenocarcinoma. Findings of 154 autopsies. Arch Surg. 1995;130(2):125-134.
doi pubmed - Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics,
2023. CA Cancer J Clin. 2023;73(1):17-48.
doi pubmed - Spetsieris N, Bobba G, Bhandari P, Patel S, Tharayil Z,
Gupta R. Pancreatic cancer with a skeletal muscle metastasis-a case presentation and literature
review. J Community Hosp Intern Med Perspect. 2022;12(5):60-64.
doi pubmed - Ayres Pereira M, Chio IIC. Metastasis in pancreatic ductal
adenocarcinoma: current standing and methodologies. Genes (Basel). 2019;11(1):6.
doi pubmed - Alfaraj D, AlOtaibi RO, Bamousa RM, Alzamami JF.
Pathological fracture as the initial presentation of metastatic pancreatic cancer. Cureus.
2022;14(1):e20920.
doi pubmed - Borad MJ, Saadati H, Lakshmipathy A, Campbell E, Hopper P,
Jameson G, Von Hoff DD, et al. Skeletal metastases in pancreatic cancer: a retrospective study
and review of the literature. Yale J Biol Med. 2009;82(1):1-6.
pubmed - Blastik M, Plavecz E, Zalatnai A. Pancreatic carcinomas in a
60-year, institute-based autopsy material with special emphasis of metastatic pattern. Pancreas.
2011;40(3):478-480.
doi pubmed - Vicic I, Belev B. The pathogenesis of bone metastasis in
solid tumors: a review. Croat Med J. 2021;62(3):270-282.
doi pubmed - McCafferty JA, Free MD, De Villiers DJ, Keith PPA. Humeral
metastases: an unusual presentation of pancreatic cancer. J Surg Case Rep.
2022;2022(5):rjac157.
doi pubmed - Saif MW, Galanina N, Ravage-Mass L, Kaley K, Cornfeld D,
Lamb L, Chhieng D. Bone metastasis as the only metastatic site in a patient with pancreatic
cancer following distal pancreatectomy. Case Rep Med. 2010;2010:634975.
doi pubmed - Okamoto M, Yamazaki H, Yoshimura Y, Aoki K, Tanaka A, Kato
H. Massive trapezial metastasis from gastric adenocarcinoma resected and reconstructed with a
vascularized scapular bone graft: A case report. Medicine (Baltimore).
2017;96(50):e9294.
doi pubmed - Song Y, Yao J. Trapezial metastasis as the first indication
of primary non-small cell carcinoma of the lung. J Hand Surg Am.
2012;37(6):1242-1244.
doi pubmed - Gaston RG, Lourie GM, Scott CC. Isolated metastatic lesion
of the trapezium. Am J Orthop (Belle Mead NJ). 2008;37(8):E144-145.
pubmed
This
article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0
International License, which permits unrestricted non-commercial use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Journal
of Medical Cases is published by Elmer Press Inc.