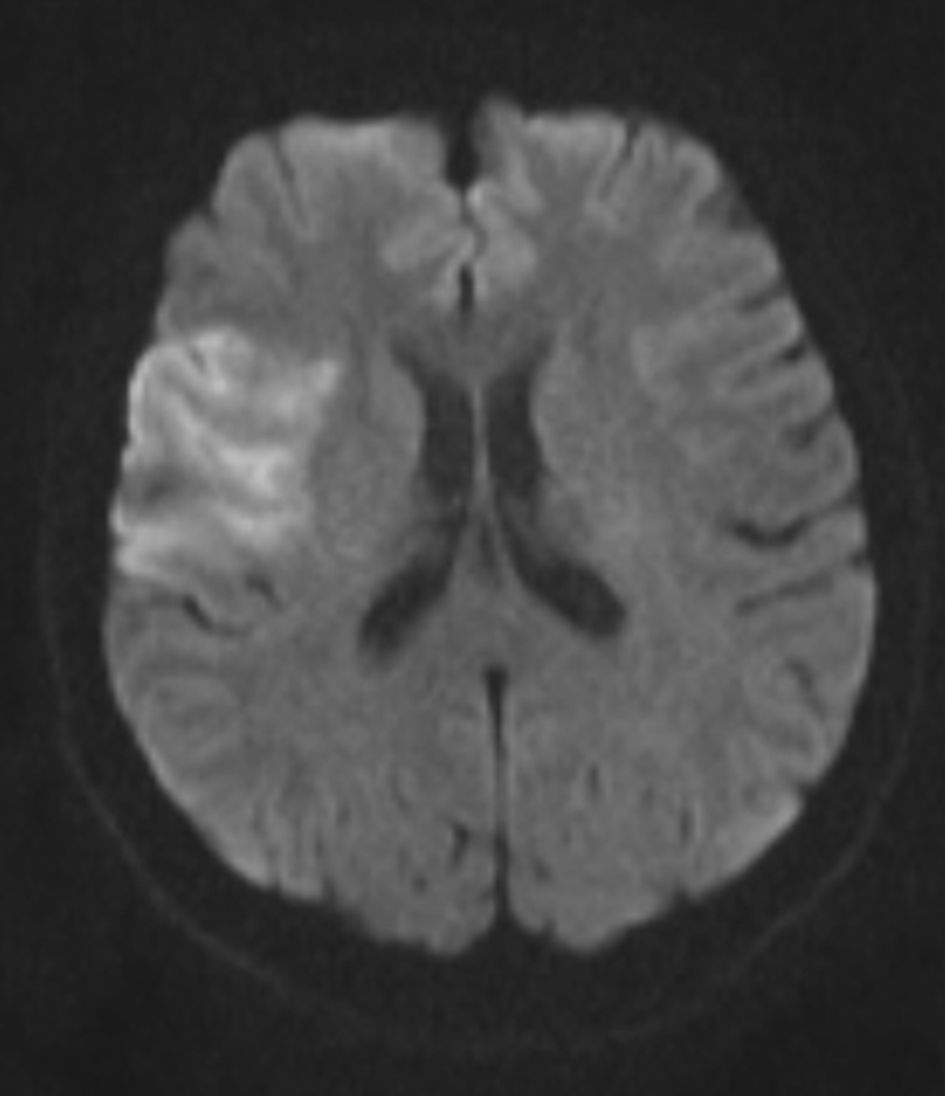
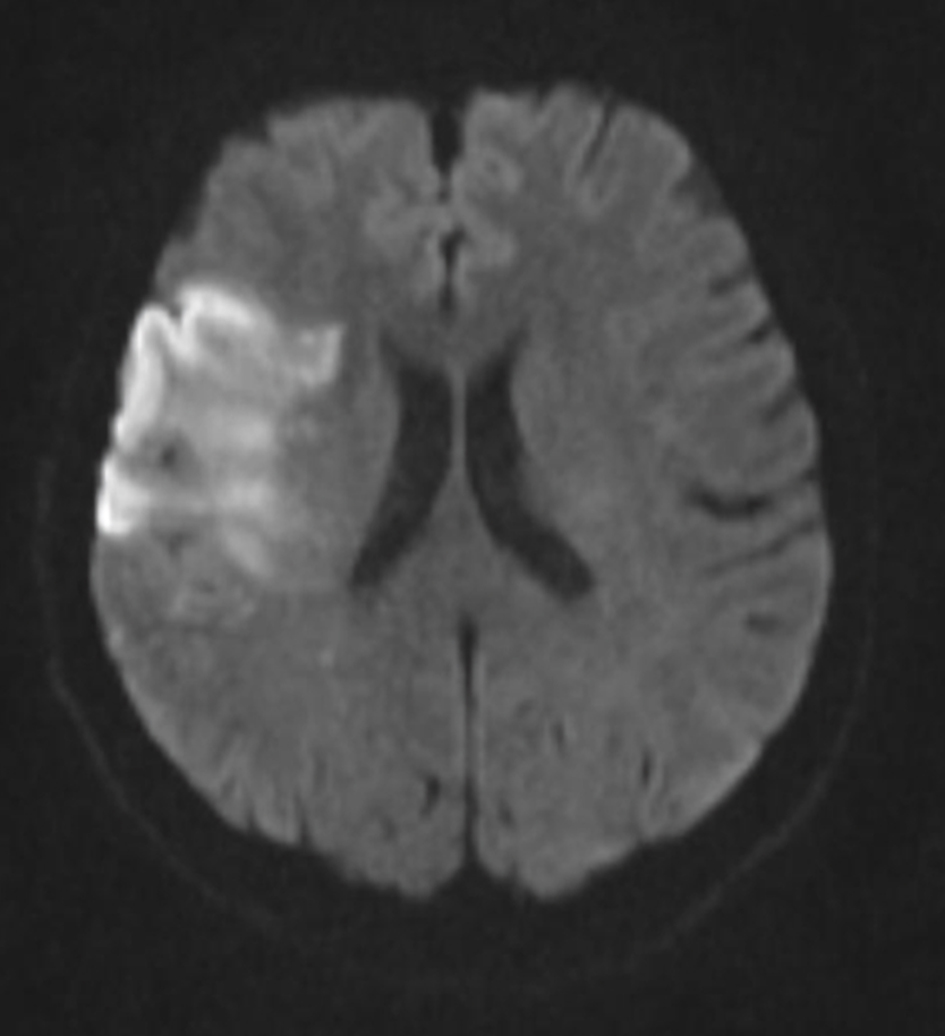
↓ Figure 1. Diffusion-weighted MRI (DWI) demonstrates signal restriction in the right frontal-insular region consistent with acute ischemic stroke. DWI: diffusion-weighted imaging; MRI: magnetic resonance imaging.
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://jmc.elmerpub.com |
Case Report
Volume 17, Number 7, July 2026, pages 356-364
Life-Saving Intracranial Mechanical Thrombectomy for Acute Ischemic Stroke in Pregnancy: Balancing Maternal and Fetal Risk
Figures

Table
| Aspect | Key points |
|---|---|
| IV: intravenous; tPA: tissue plasminogen activator; CT: computed tomography; BP: blood pressure; CVST: cerebral venous sinus thrombosis; RCVS: reversible cerebral vasoconstriction syndrome. | |
| Incidence | About 10–30 per 100,000 pregnancies; highest in peripartum/postpartum |
| Initial step | Immediate neuroimaging (noncontract CT); do not delay |
| IV thrombolysis (tPA) | Within 4.5 h; pregnancy not absolute contraindication; individualized risk–benefit |
| Mechanical thrombectomy | Indicated for large-vessel occlusion; safe in selected pregnant patients |
| Anticoagulation (acute phase) | Not recommended (increase hemorrhagic transformation risk) |
| Secondary prevention | Antiplatelet therapy after acute phase |
| Supportive care | Control BP, glucose (140–180 mg/dL), normothermia, avoid hypotonic fluids |
| Special etiologies | Manage CVST, dissection, RCVS per standard guidelines |
| Core principle | Treat as standard stroke with pregnancy-specific considerations |