↓ Figure 1. Physical examination of the patient revealed a 25-mm soft, non-pulsatile mass in the right antecubital fossa. Tenderness and the absence of a bruit were also noted.

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://jmc.elmerpub.com |
Case Report
Volume 17, Number 7, July 2026, pages 348-355
Cephalic Venous Aneurysm and Intravascular Papillary Endothelial Hyperplasia in a Blood Donor
Figures
Table
| Author/year | No. | Anticoagulation | Age (years)/sex/vein | Etiology/onset | Clinical presentation | Size (mm) | Imaging | Treatment | Follow-up | Histopathology |
|---|---|---|---|---|---|---|---|---|---|---|
| IPEH: intravascular papillary endothelial hyperplasia; MRI: magnetic resonance imaging; US: ultrasound; VA: venous aneurysm; VPA: venous pseudoaneurysm. | ||||||||||
| Niimi et al, 2017 [16] | 1 | No | 58/female/right basilic vein | Blood sampling/3 years | Non-pulsatile antecubital mass with compression of the lateral antebrachial cutaneous nerve | 24 × 19 | Duplex US, MRI: VPA with thrombus | Persistent thrombus despite anticoagulation Successful surgical resection with ligation | 2 years; no recurrence | VPA: dilatation with a thickened intima and media |
| 2 | No | 56/female/left basilic vein | Venipuncture/2 months | Non-pulsatile antecubital mass | 23 × 17 | Duplex US, MRI: VPA | Successful surgical resection | 6 months; no recurrence | VPA: dilatation with thrombus | |
| Ward et al, 2009 [14] | 3 | Yes | 64/male/right basilic vein | Venipuncture/immediately | Non-pulsatile antecubital mass | 40 × 30 position-dependent | B-mode and duplex US: 43 × 33 × 20 mm cavity with low-pressure swirling flow | Unsuccessful compression Successful surgical resection with ligation | n/a | VPA: lack of endothelial lining |
| Lotfi et al, 2007 [10] | 4 | No | 43/male/left median antecubital vein | Venipuncture for blood donation/immediately | Non-pulsatile, tender antecubital mass | 30 position-dependent | US: 30 × 15 mm cystic lesion with thrombosis Doppler analysis: swirling flow | Successful surgical resection and repair of the puncture site | n/a | VPA: lack of vascular wall with granulation tissue and thrombosis |
| Chakraborty et al, 1999 [13] | 5 | Yes | 57/female/left antecubital vein | Venipuncture/immediately | Non-pulsatile, tender antecubital mass | 45 | US, venography: compressible VPA | Successful embolization | 6 weeks; no recurrence | n/a |
| Debnath et al, 2007 [5] | 6 | No | 45/female/right median cubital vein | Peripheral intravenous line/few months | Non-pulsatile, non-tender antecubital mass | 20 × 30 | Duplex US: VA | Successful surgical resection with ligation | n/a | VA: preservation of three layers, thickened media, and congested lumen |
| Perler, 1990 [15] | 7 | No | 39/female/unspecified | Peripheral intravenous line/immediately | Non-pulsatile, non-tender wrist mass | 35 × 15 | Venous Doppler analysis; normal Venography: VA | Surgical resection with ligation | n/a | VA |
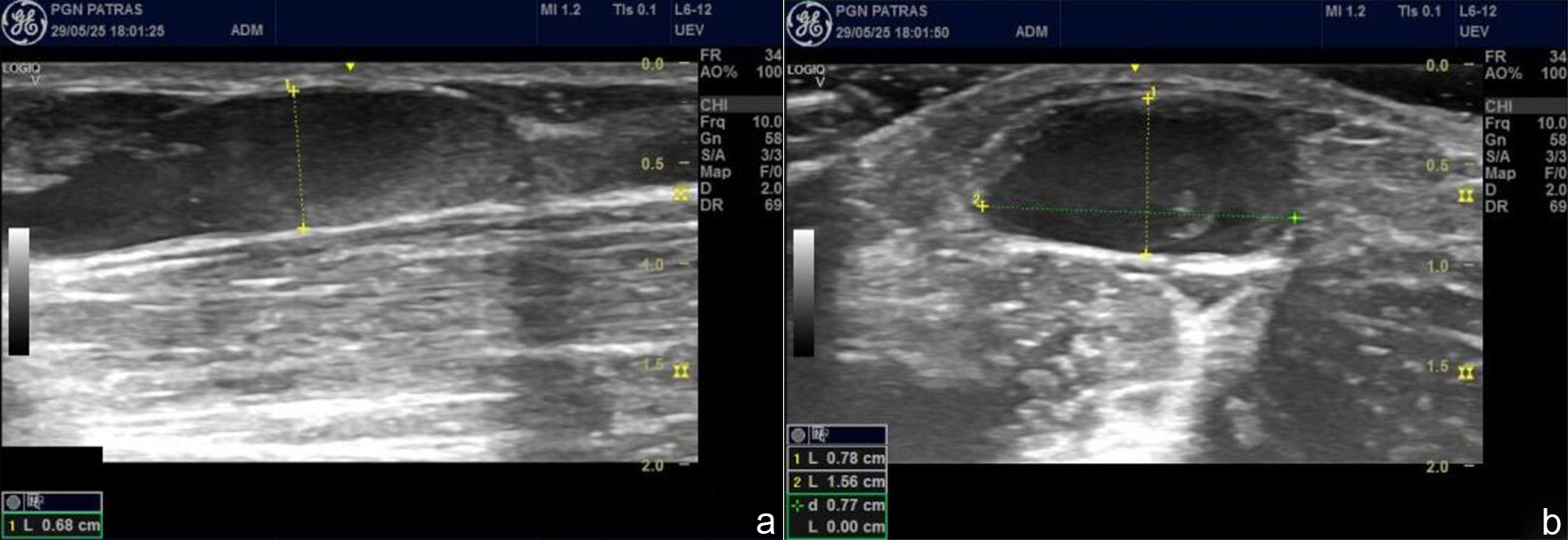
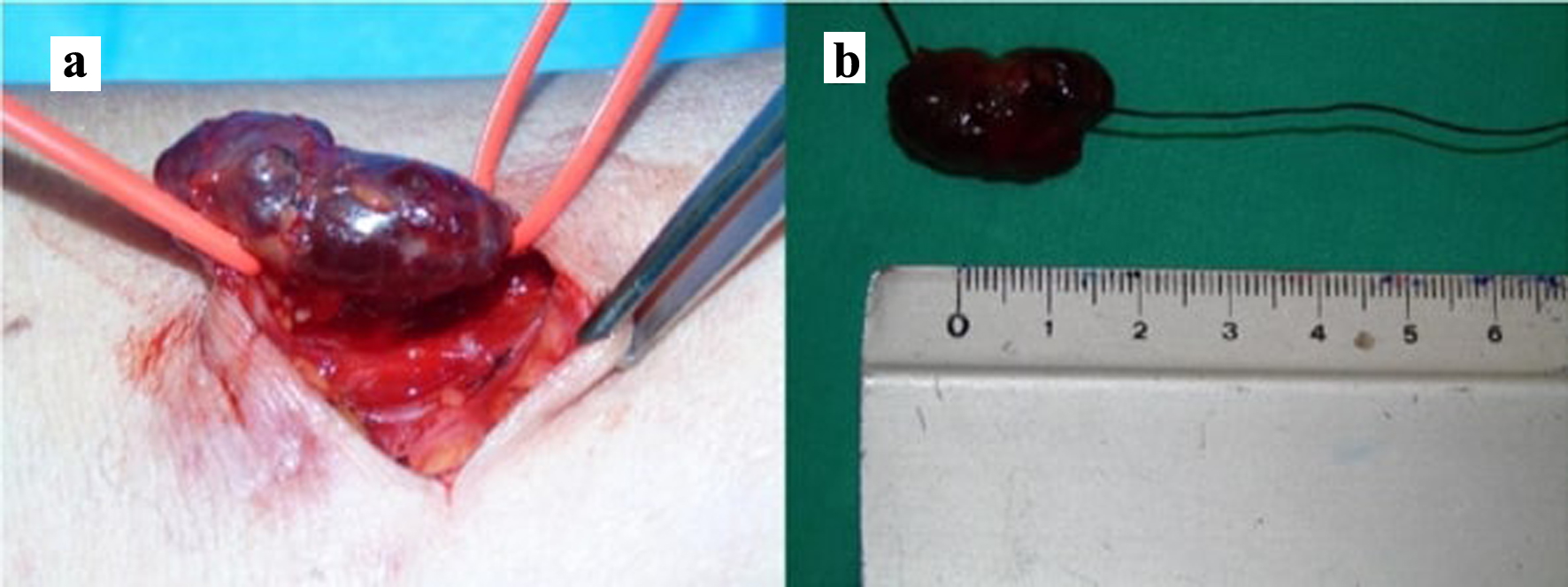
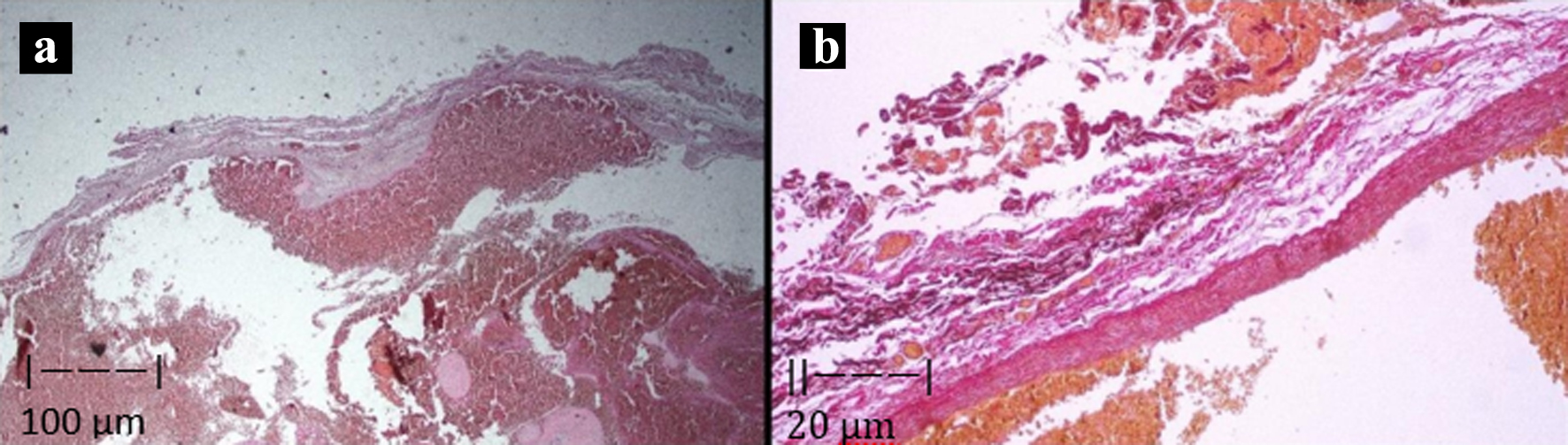
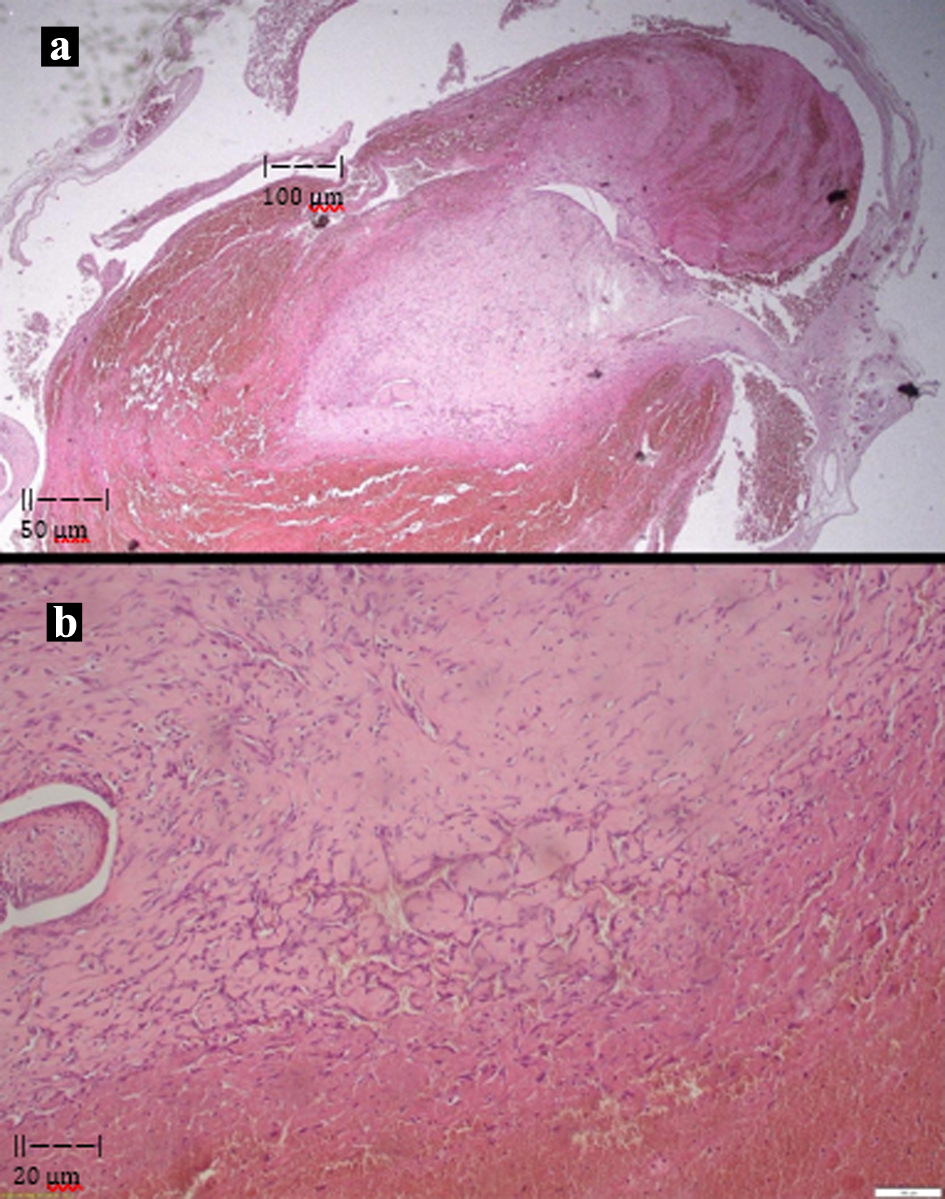
| Our case | 8 | No | 52/male/right cephalic vein | Venipuncture for blood donation/unspecified | Non-pulsatile, tender antecubital mass | 25 position-dependent | Duplex US: saccular dilation (15.6 × 7.8 × 25.5 mm) with thrombus | Anticoagulation and surgical resection with ligation | 2 weeks; no recurrence | VA: dilation of the vascular lumen with disorganization of the vascular wall; endophlebosclerosis and IPEH |