| 5 months prior |
Intermittent fever, lower back pain. Blood culture: Brucella
melitensis |
Rifampicin + ciprofloxacin for 6 weeks. |
6 |
- |
1:320 |
Symptom resolution |
| 2 months post-treatment (admission) |
Recurrent fever, malaise, 10 kg weight loss, followed by acute left-sided
hemiparesis. |
Hospital admission, diagnostic workup. |
12 |
0.20 |
1:40 → 1:160 |
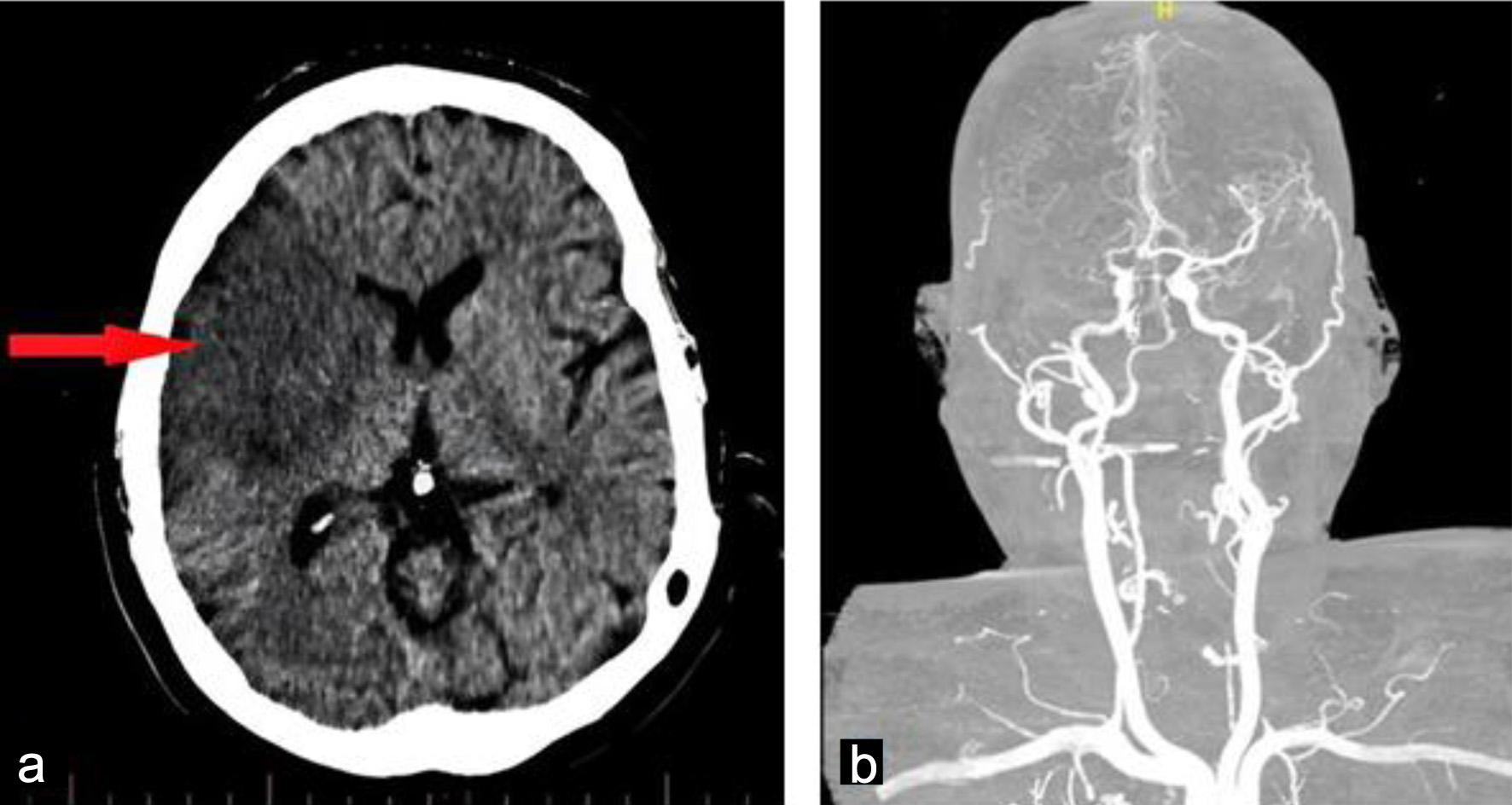
Embolic stroke confirmed on CT. |
| During inpatient phase (weeks 1–8) |
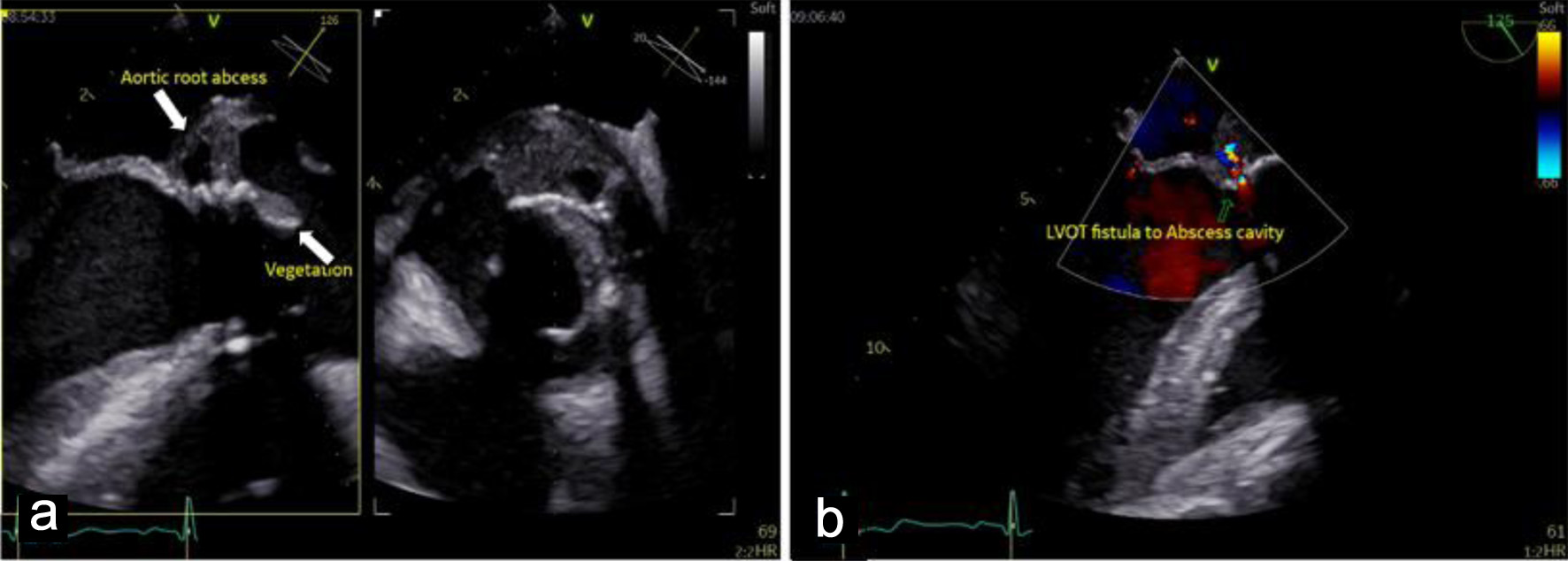
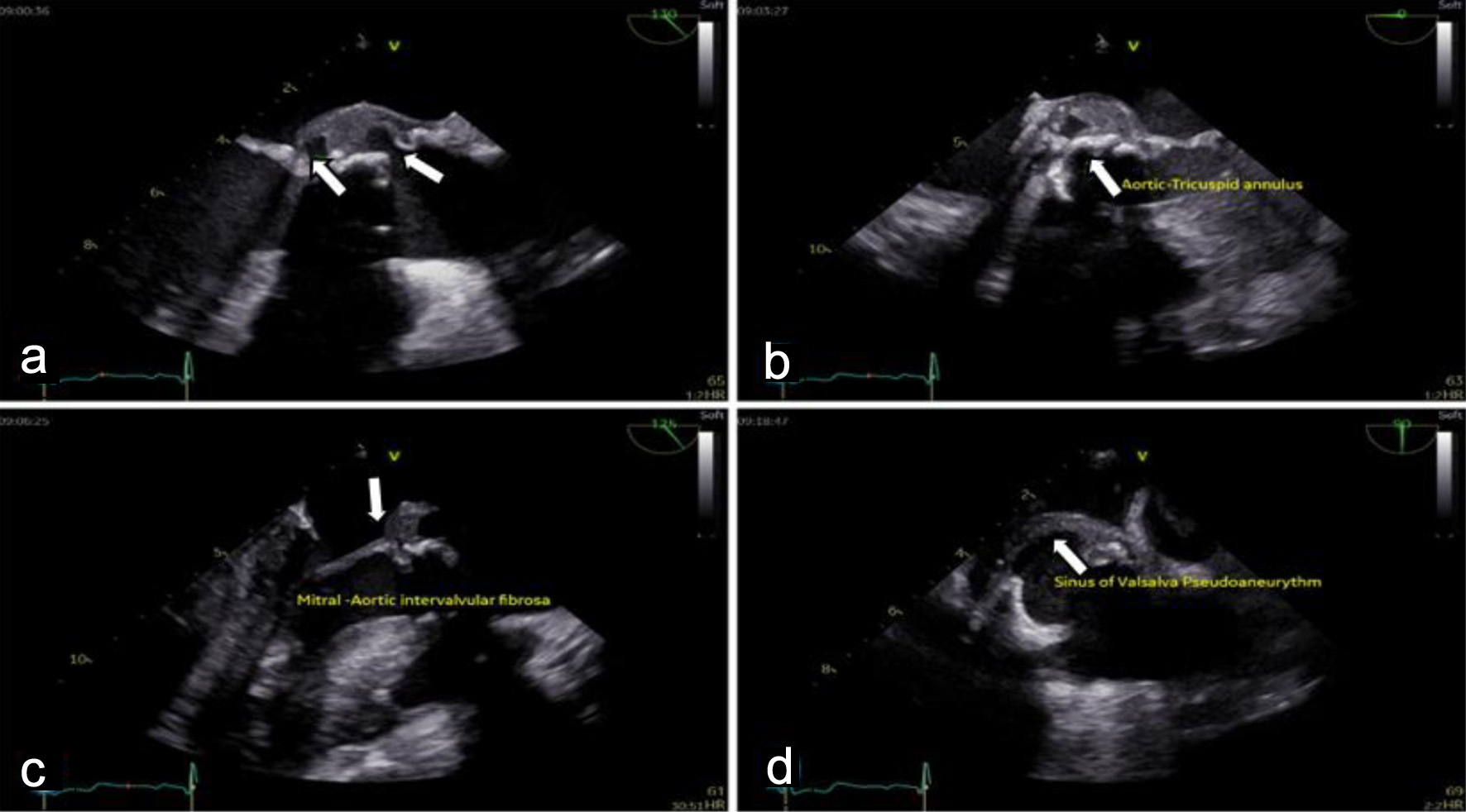
Diagnosis of BE with paravalvular abscess and spondylitis. Patient
declined surgery. |
Initiated quadruple therapy: rifampicin, doxycycline, gentamicin, TMP-SMX.
Inpatient monitoring. |
14 → 10 → 3.37 |
0.01 → 0.03 |
1:320 |
Fever and back pain resolved. Neurological improvement. Echo: vegetation
and abscess regressing. |
| Post-discharge (months 3–9) |
Outpatient follow-up. Gentamicin was discontinued after the initial phase.
|
Continued oral therapy: rifampicin, doxycycline, TMP-SMX. Bi-weekly
clinical and lab follow-up. |
1.7 |
0.05 |
1:80 |
Clinically stable, afebrile. Independent in daily activities. |
| 6-month follow-up |
Asymptomatic. No signs of heart failure or infection relapse. |
Completion of a prolonged antimicrobial course. Final echocardiogram. |
Normal |
Normal |
1:40 (baseline) |
Complete resolution: No vegetation/abscess on echo. Preserved valve
function. No relapse. |