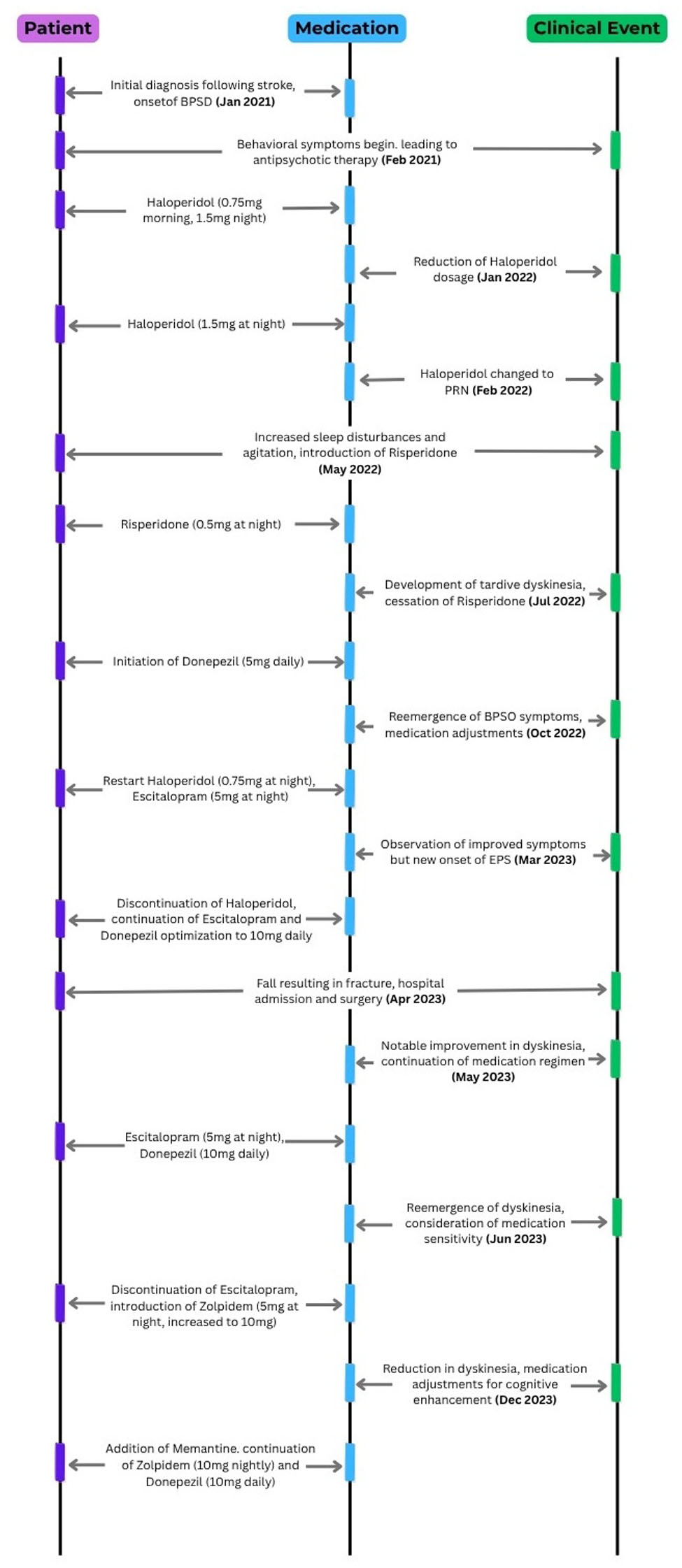
↓ Figure 1. Event and medication.
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://jmc.elmerpub.com |
Case Report
Volume 17, Number 6, June 2026, pages 244-250
Tardive Oropharyngeal Dyskinesia Associated With Antipsychotic Use in the Management of Behavioral and Psychological Symptoms of Dementia
Figures
Table
| Risk category | Medication class | Examples | Key notes |
|---|---|---|---|
| Medications associated with TD and EPS, categorized according to relative risk based on available literature. Risk stratification reflects general trends reported in the literature and may vary depending on patient factors such as age, comorbidities, duration of exposure, and polypharmacy. APDs: antipsychotic drugs; L-DOPA: L-3,4-dihydroxyphenylalanin; LID: L-DOPA-induced dyskinesia; MAO: monoamine oxidase; SSRIs: selective serotonin uptake inhibitors; TCAs: tricyclic antidepressants. | |||
| High risk | Typical antipsychotics | Haloperidol | Strong D2 blockade; highest association with TD and EPS |
| Dopamine antagonist antiemetics | Metoclopramide, prochlorperazine | Significant TD risk, especially with prolonged use (> 12 weeks) | |
| Moderate risk | Atypical antipsychotics | Risperidone, olanzapine, aripiprazole | Lower risk than typical APDs but still associated; some agents reported to induce TD |
| Antidepressants | SSRIs (fluoxetine, sertraline), TCAs (amitriptyline, clomipramine) | Risk higher in older adults and with long-term exposure | |
| MAO inhibitors | Selegiline, rasagiline, phenelzine | Associated with dyskinesia, especially with dopaminergic interaction | |
| Mood stabilizers | Lithium (especially with APDs) | Increased risk when combined with antipsychotics | |
| Low but notable risk | Anticholinergics | Procyclidine, trihexyphenidyl | May worsen TD and cognitive impairment |
| Anticonvulsants | Phenytoin, carbamazepine, lamotrigine | Rare but reported; possibly underdiagnosed | |
| Antihistamines | Hydroxyzine | Risk with prolonged use, especially in older adults | |
| Antiparkinsonian drugs | L-DOPA | Dyskinesia (LID), dose- and duration-related | |
| Rare/context-dependent risk | Decongestants | Pseudoephedrine, phenylpropanolamine | May exacerbate movement disorders |
| Antimalarials | Chloroquine, amodiaquine | Mechanism unclear; possible neurotransmitter disruption | |
| Anxiolytics | Benzodiazepines (withdrawal), barbiturates | Withdrawal-emergent dyskinesia | |
| Stimulants | Amphetamines, methamphetamine | Dopaminergic neurotoxicity; persistent dyskinesia possible | |