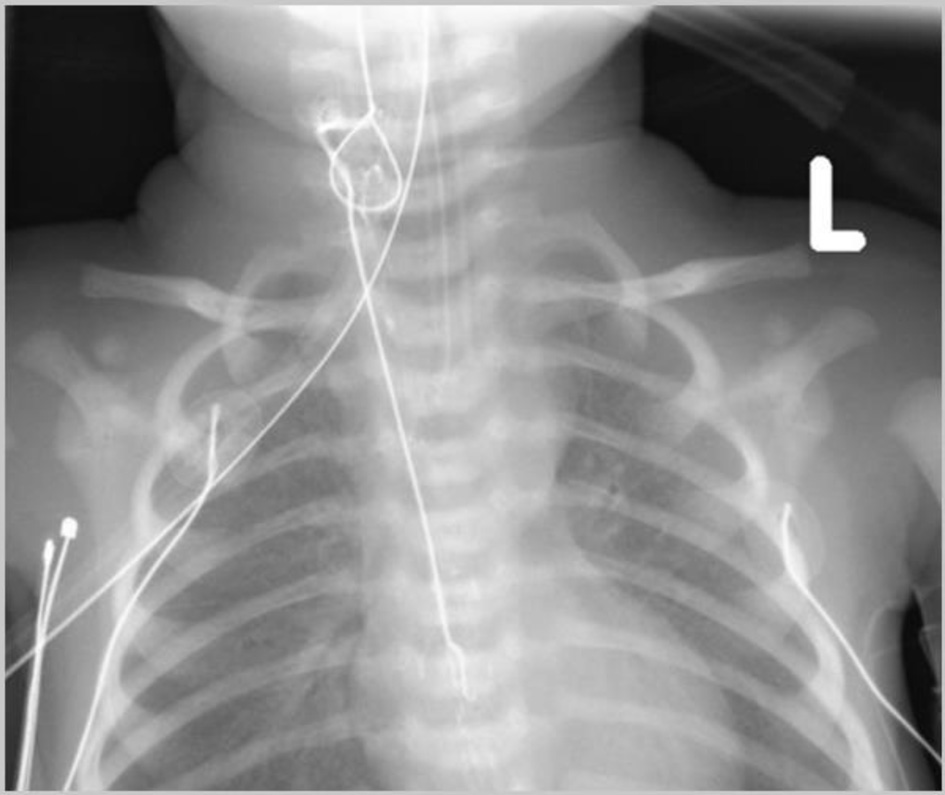
↓ Figure 1. Initial intraoperative chest
radiograph revealing looping of the nasogastric (NG) tube within the esophagus and its tip in the fundus
of the stomach.

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://jmc.elmerpub.com |
Case Report
Volume 17, Number 3, March 2026, pages 128-132
Misplaced and Knotted Nasogastric Tubes in Infants and Children: Report of Two Cases
Figures

Tables
| ETT: endotracheal tube; NG: nasogastric. |
| Use of narrow bore tubes |
| Excessive tube length in the stomach |
| Gastric anatomy including small stomach volumes |
| Altered gastric anatomy following surgery |
| Vigorous peristalsis activity |
| Prolonged duration of tube placement |
| Excessive tube manipulation or movement |
| Rapid insertion or withdrawal of the ETT |
| AP: anteroposterior; NG: nasogastric. |
| 1. High index of suspicion when excessive resistance is noted on attempted NG tube removal. |
| 2. Attempts at withdrawal should stop—never pull against resistance due to risk of esophageal or airway injury. |
| 3. Imaging studies (lateral/AP neck or skull radiograph) may identify the knot and its position. |
| 4. Attempt to visualize the knot in the oropharynx. If it can be seen, it may be possible to hold the knot with a forceps and cut above it. |
| 5. The knot is then removed through the mouth with the distal end of the NG while the remainder of the NG tube (proximal end) is removed through the nare. |
| 6. If the knot is more distal, removal under direct vision with sedation/anesthesia may be required. This may require consultation with otolaryngology or gastroenterology. |