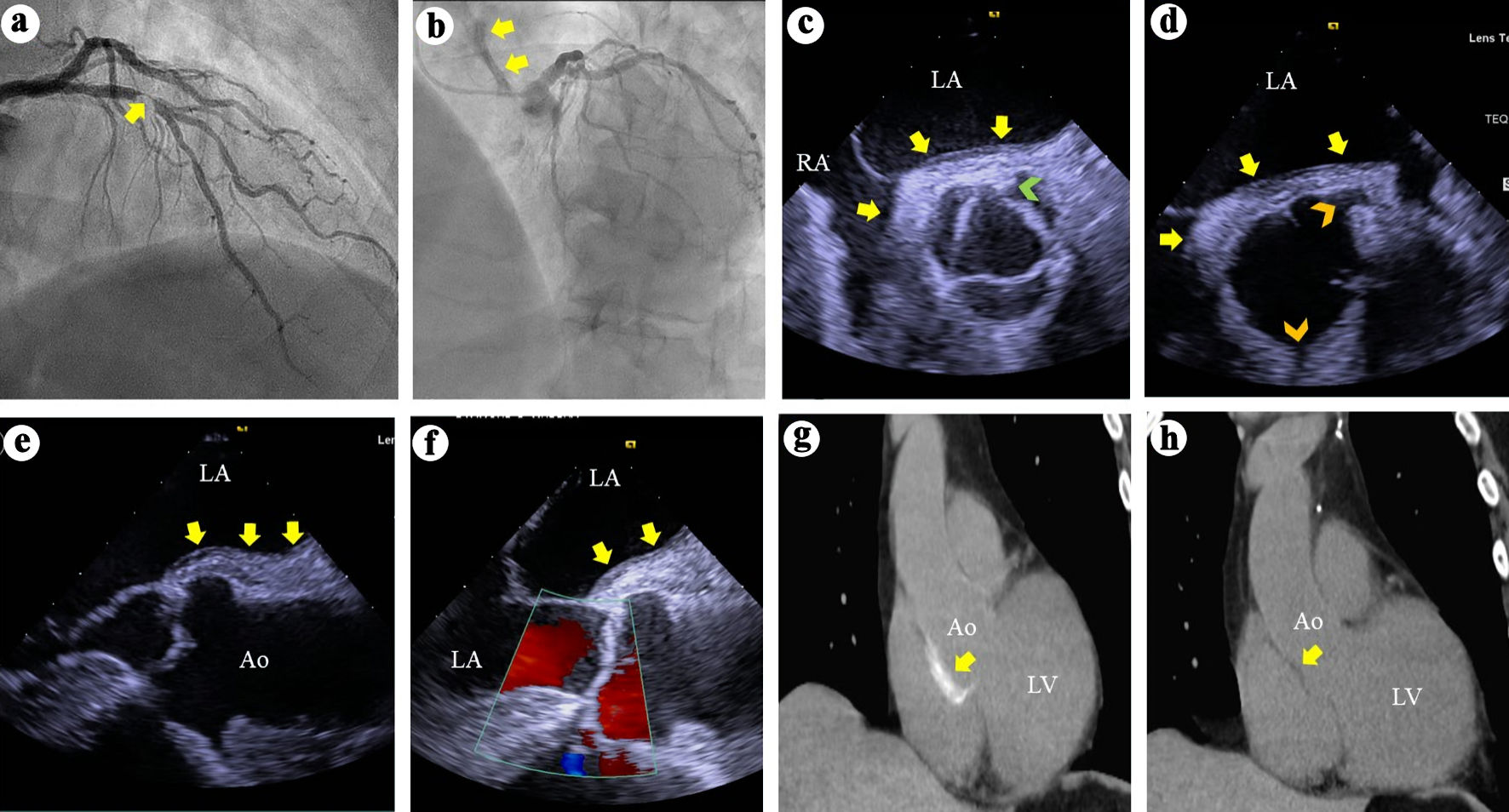
↓ Figure 1. (a) Right anterior oblique view of
the left coronary arteries angiography demonstrates a > 95% complex stenosis (arrow) of the left
anterior descending coronary artery. (b) Left anterior and cranial view of the left coronary system
demonstrates contrast hang-up or staining (arrows) on the aortic root and ascending aorta. (c) TEE short
axis views at the aortic valve level during systole demonstrates soft tissue echo-reflectant thickening
of the aortic root posterior wall with medial and lateral extensions (arrows) and a possible small
intimal tear (green arrowhead). (d) TEE short-axis view of the aortic root during diastole demonstrates
aortic wall thickening (arrows) and intact ostial left main and right coronary arteries (top and bottom
arrowheads, respectively). (e, f) TEE long-axis views demonstrate soft tissue thickening of the
posterior aortic root and ascending aortic wall (arrows) and intact aortic valve with no regurgitation.
(g) Thoracic CT demonstrates contrast uptake at the aortic root and part of the ascending aorta (arrow).
(h) Repeat thoracic CT 7 weeks later demonstrates resolution of the contrast uptake at the aortic root
and ascending aorta. TEE: transesophageal echocardiography; CT: computed tomography; LA: left atrium;
RA: right atrium; Ao: aorta; LV: left ventricle.