Figures
↓ Figure 1. Mid-esophageal four-chamber view. A
mass with lateral wall stalk prolapses through mitral valve during diastole. The arrow denotes the large
cardiac tumor.

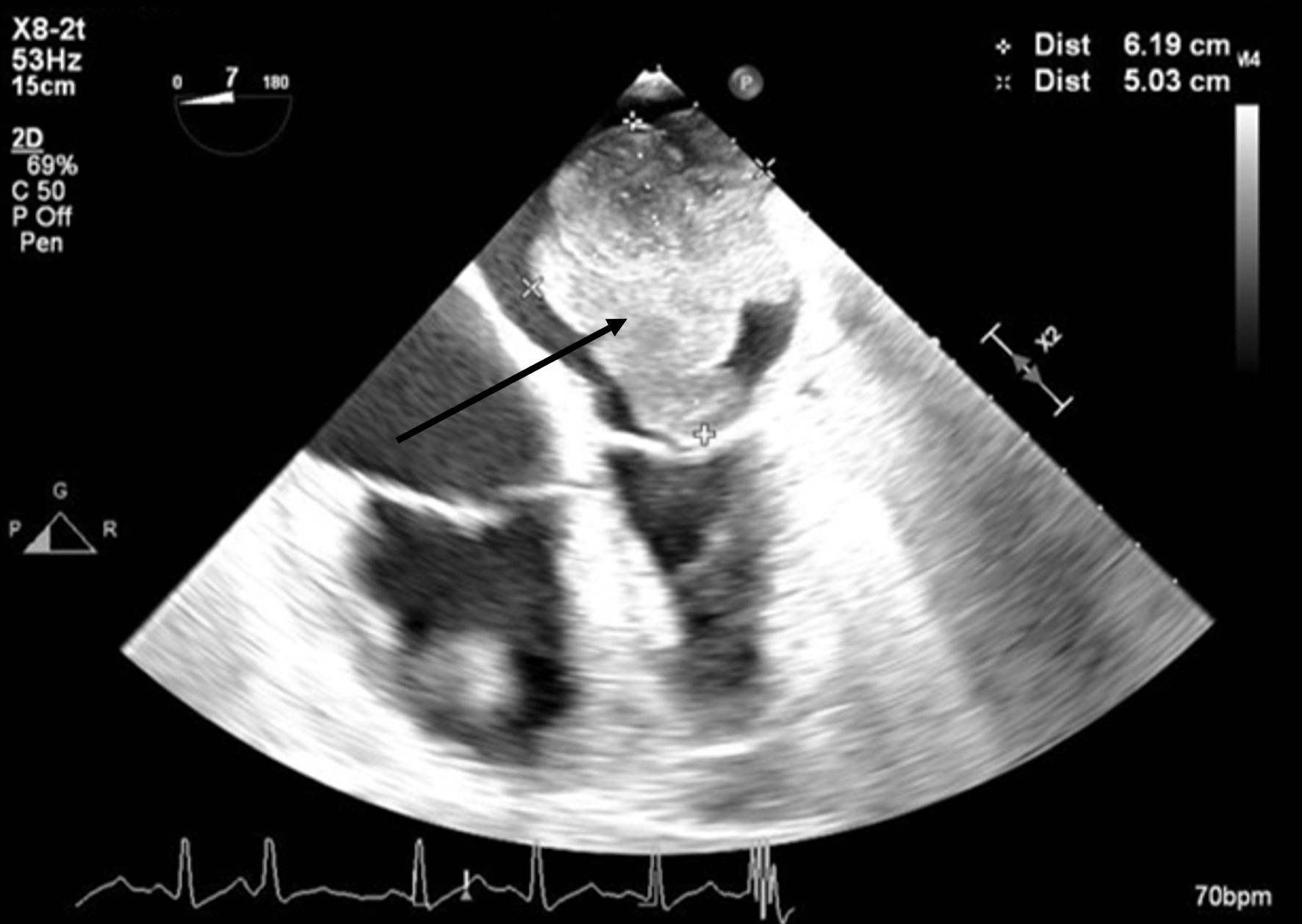
↓ Figure 2. Mid-esophageal four-chamber view. A
mass occupies the majority of the left atrium during systole. The arrow denotes the large cardiac
tumor.
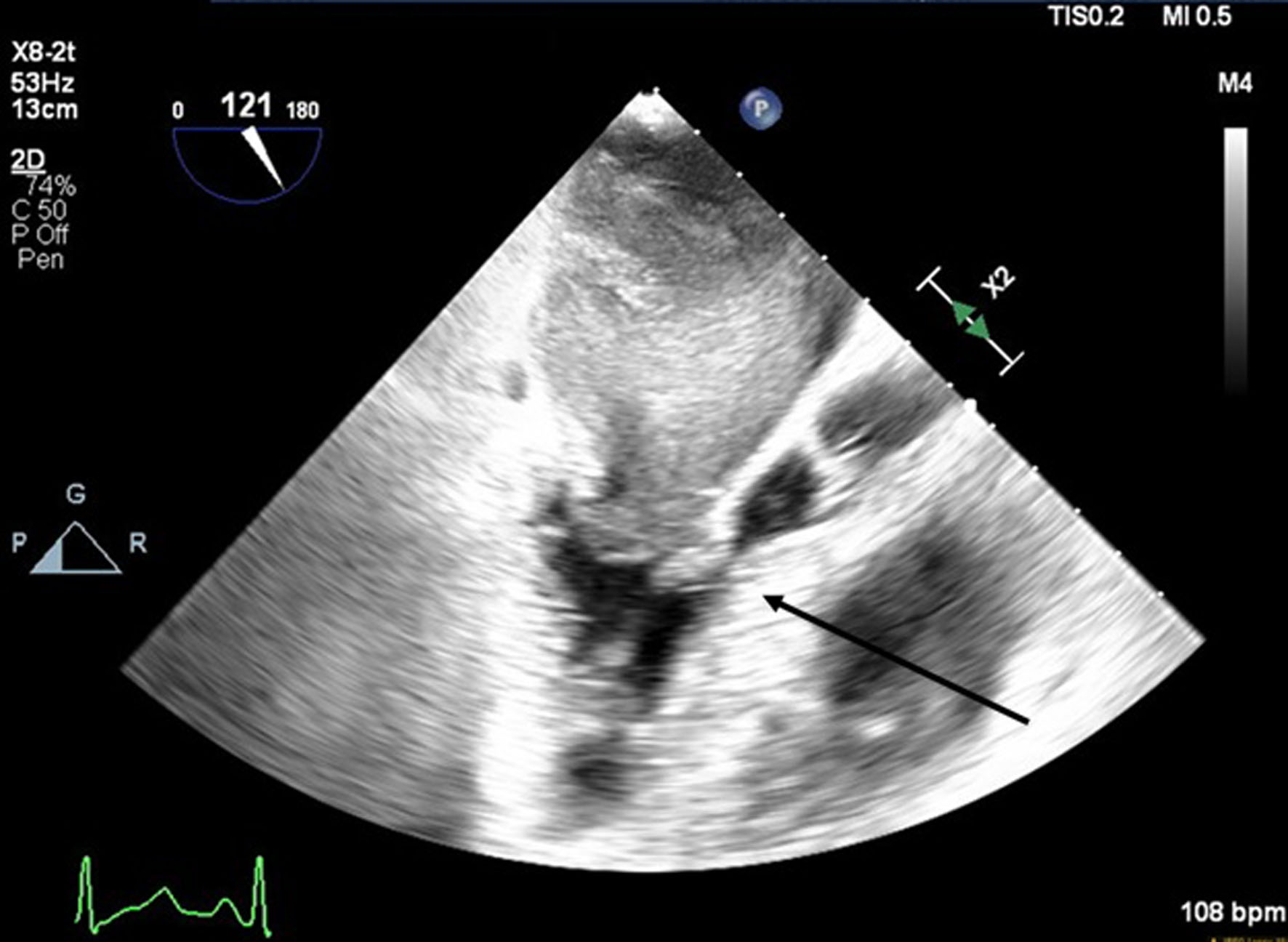
↓ Figure 3. Mid-esophageal aortic long-axis view
showing a mass obstructing the left ventricular outflow tract (LVOT) during early systole. The arrow
indicates LVOT obstruction.
↓ Figure 4. Mid-esophageal two-chamber view with
color flow Doppler demonstrating turbulent flow around the mass through the mitral valve during
diastole. The arrow indicates turbulent flow through the mitral valve.
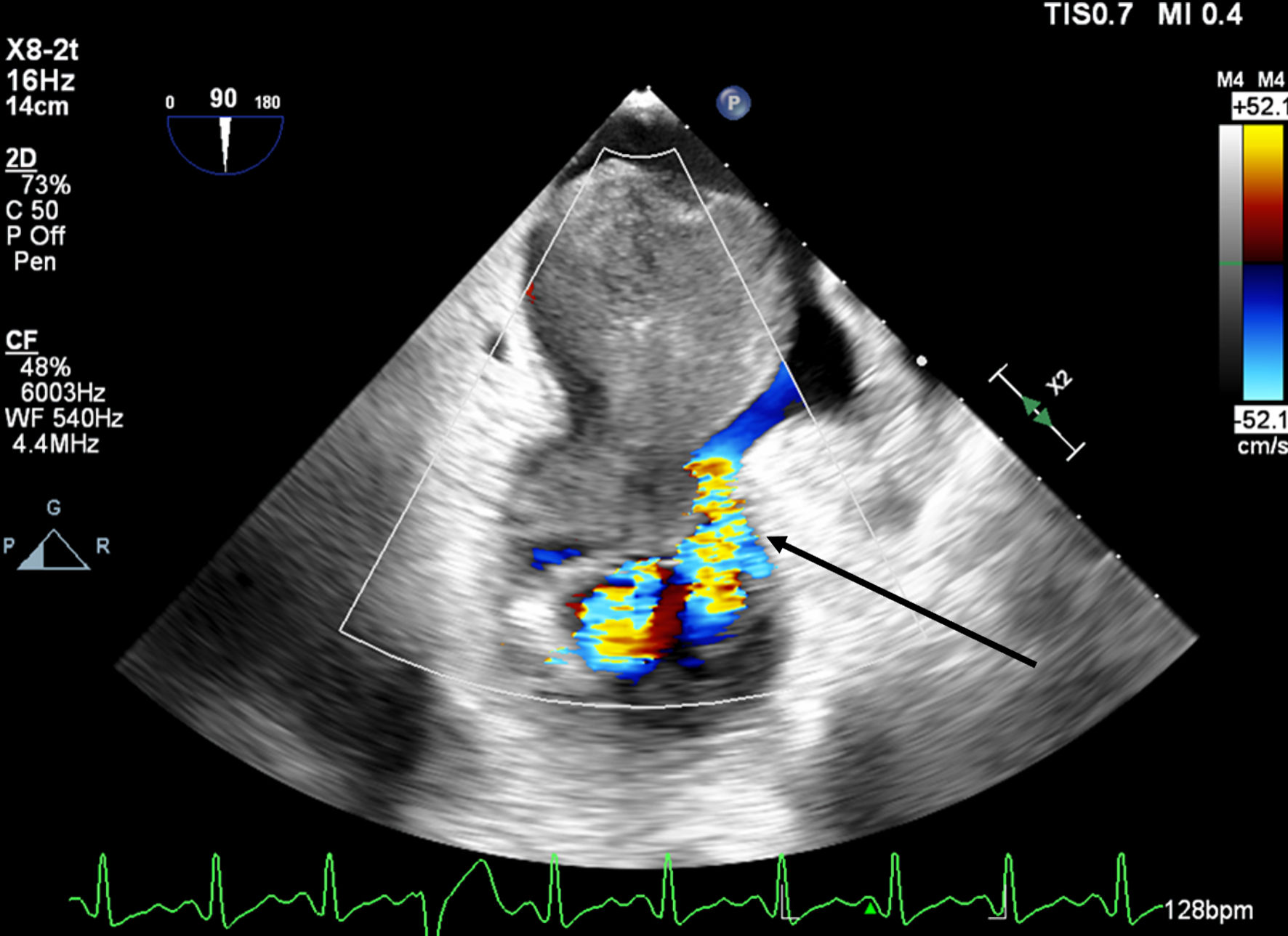
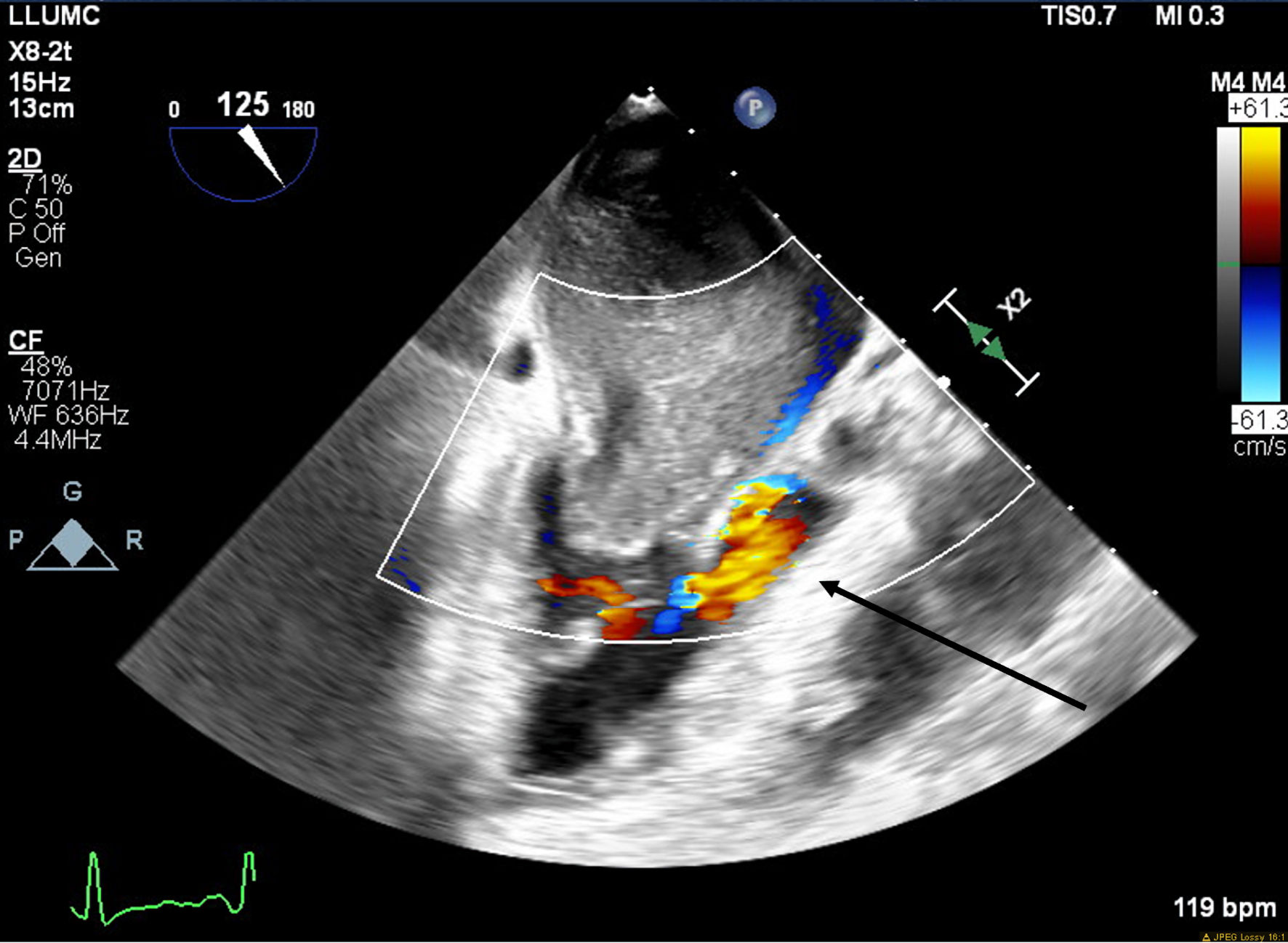
↓ Figure 5. Mid-esophageal aortic long-axis view
with color flow Doppler demonstrating turbulent flow through left ventricular outflow tract (LVOT)
during early systole. The arrow indicates turbulent flow through the LVOT.
↓ Figure 6. Photograph of the mass following
resection.

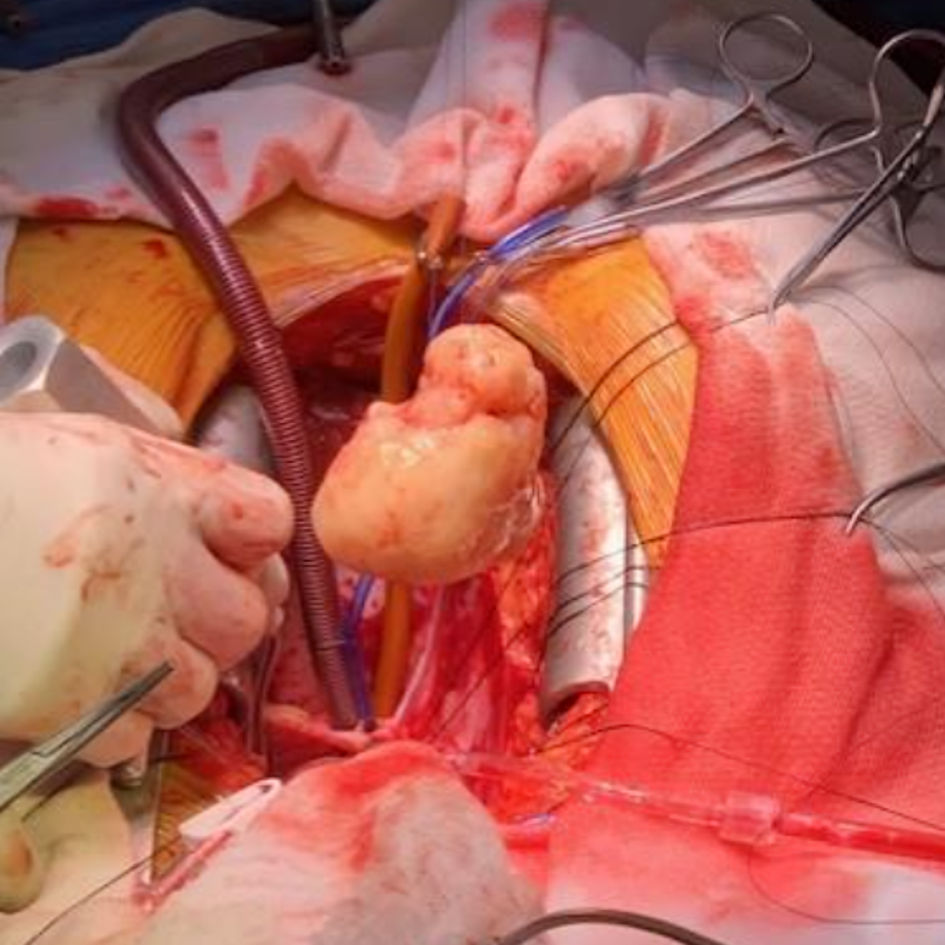
↓ Figure 7. Photograph of the mass following
resection during surgery.
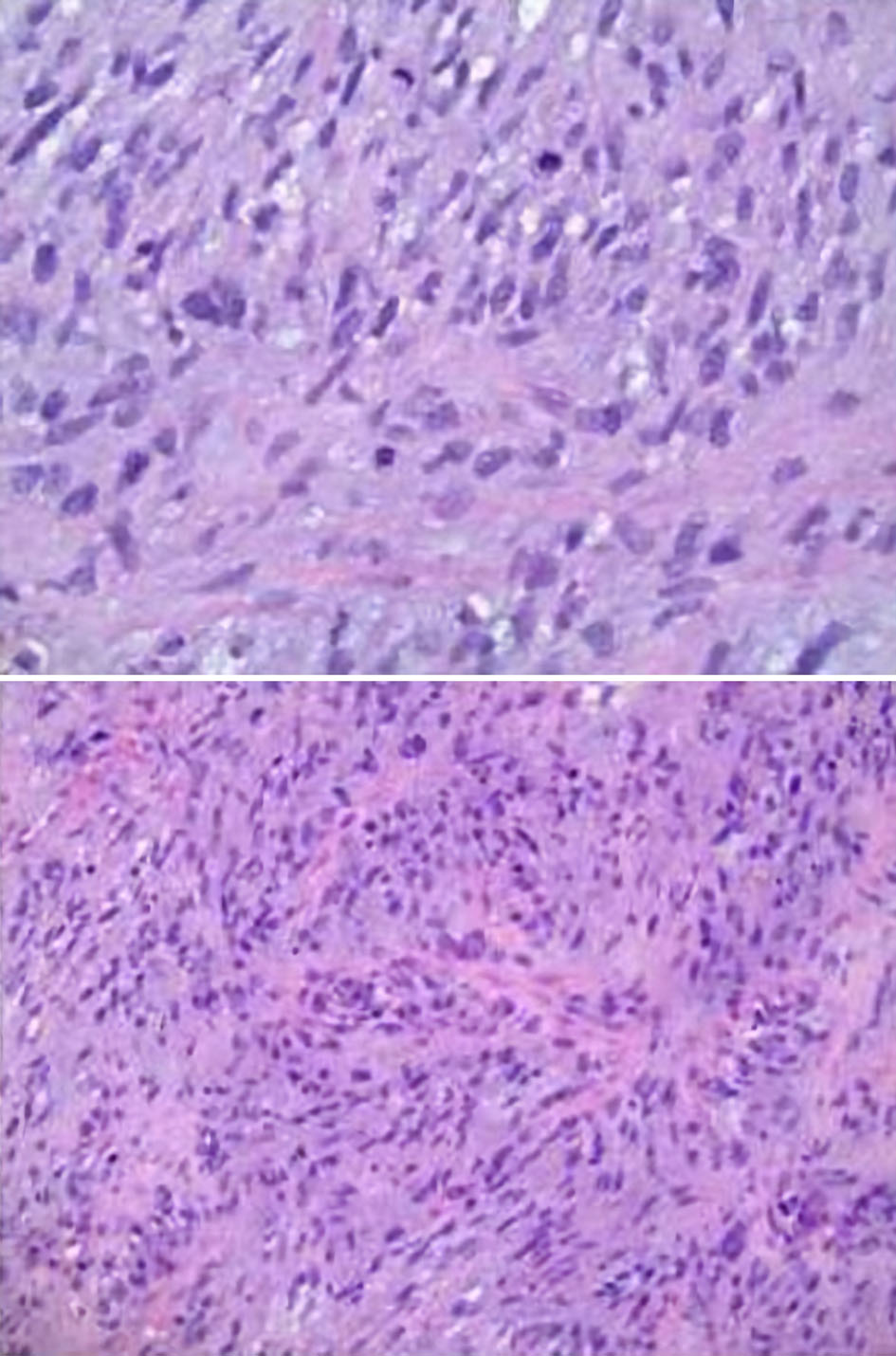
↓ Figure 8. Microscopic pathology images
demonstrating cardiac undifferentiated pleomorphic sarcoma (UPS), grade 3. The histology displays
variable cellularity, with areas of marked pleomorphism, as well as foci of myxoid change and focal
necrosis. Mitoses are easily identified in some areas and are scarce in others. These features support
the interpretation of an UPS.