| [1] |
55/F |
Unstable multilevel cervical injuries: C1 anterior arch; bilateral pedicle
fractures C3-C6; C5 body fracture; laminar and transverse-foramen involvement. |
No |
Managed nonoperatively with halo vest → stable by 4 months;
asymptomatic at 4-year follow-up with CT showing healed/sclerotic fracture lines and normal
alignment. |
| [2] |
21/F |
Subacute type II odontoid (C2 dens) fracture with C1-C2 instability |
Yes |
Posterior C1-C2 fusion (transarticular screws + interspinous wiring +
iliac crest graft); Miami-J 3 months; solid/stable fusion at 2-year follow-up, mild ROM limitation.
|
| [3] |
63/M |
C1 anterior arch fracture detected 1 week post-C1 laminectomy;
preoperative ADI 6.68 mm (AAS); TAL intact; peri-fracture hemorrhage on MRI; later calcification of
the TAL. |
No |
Nonoperative: Philadelphia collar; pseudoarthrosis at 1 year (collar
stopped); partial gap fill by 3 years, persistent painless nonunion at 5-year follow-up; no surgery
needed, asymptomatic and stable. |
| [4] |
27/M |
No vertebral fracture described; traumatic central cord syndrome on MRI
with congenitally stenotic cervical canal. |
Yes |
C3-C7 laminoplasty; spine hardware stable at 6 weeks and 3 months; patient
then lost to follow-up, reported no issues at departure. |
| [5] |
76/F |
C2 traumatic spondylolisthesis (Levine-Edwards type II hangman’s)
with severe translation; osteopetrotic bone dense, cancellous bone absent. |
Yes |
Anterior C2-3 discectomy/reduction and plated interbody fusion using
titanium-coated PEEK cage + synthetic graft; drilling with high-speed burr, minor C2 corner fracture
during tapping, managed intraoperatively; collar × 6 months total; solid union at 1 year. |
| Ours |
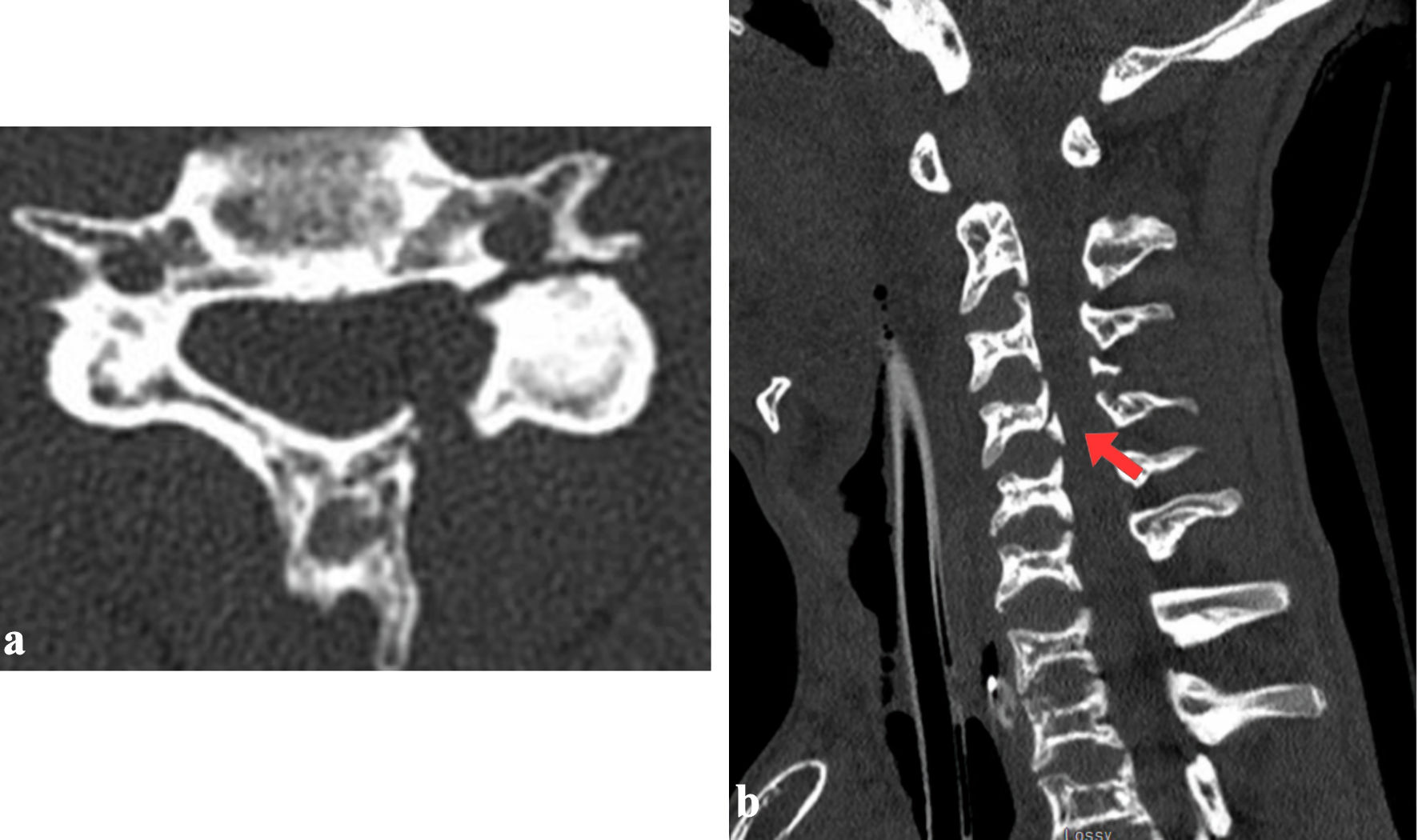
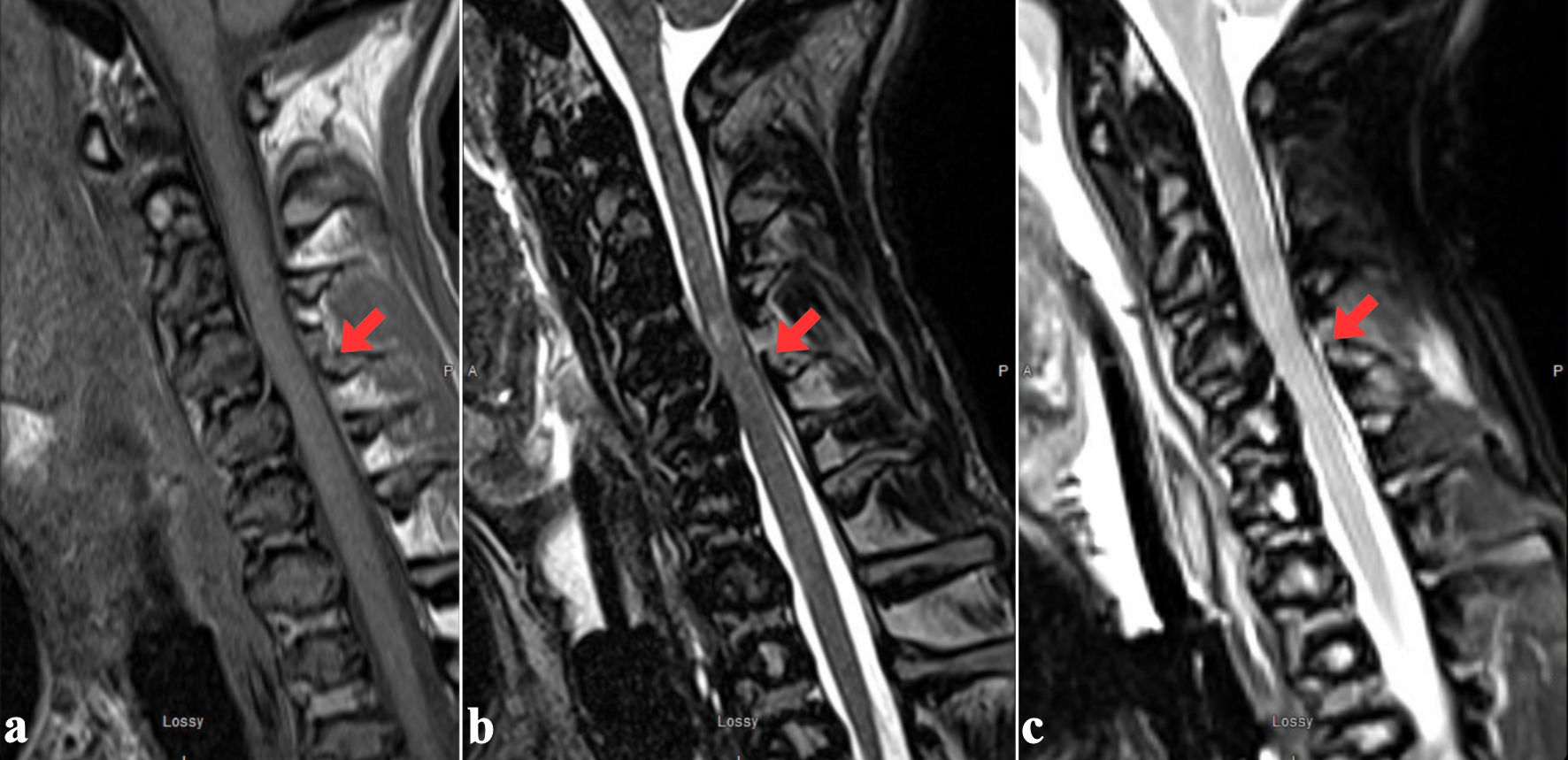
22/M |
Displaced fracture of the posterior C4 vertebral body and a complex
fracture of the left C4 lateral mass (involving the pedicle, lamina, transverse foramen, and both
articular facets). Nondisplaced fractures of the left C6 pedicle and the left C3 inferior facet. MRI
confirmed a spinal cord contusion at the C3-4 level, evidenced by a focal T2-hyperintense signal. It
also revealed significant ligamentous injury, including damage to the posterior longitudinal
ligament at C4, attenuation of the ligamentum flavum at C3-4, traumatic widening of the left C3-4
facet joint, and a small C4-5 epidural hematoma. |
No |
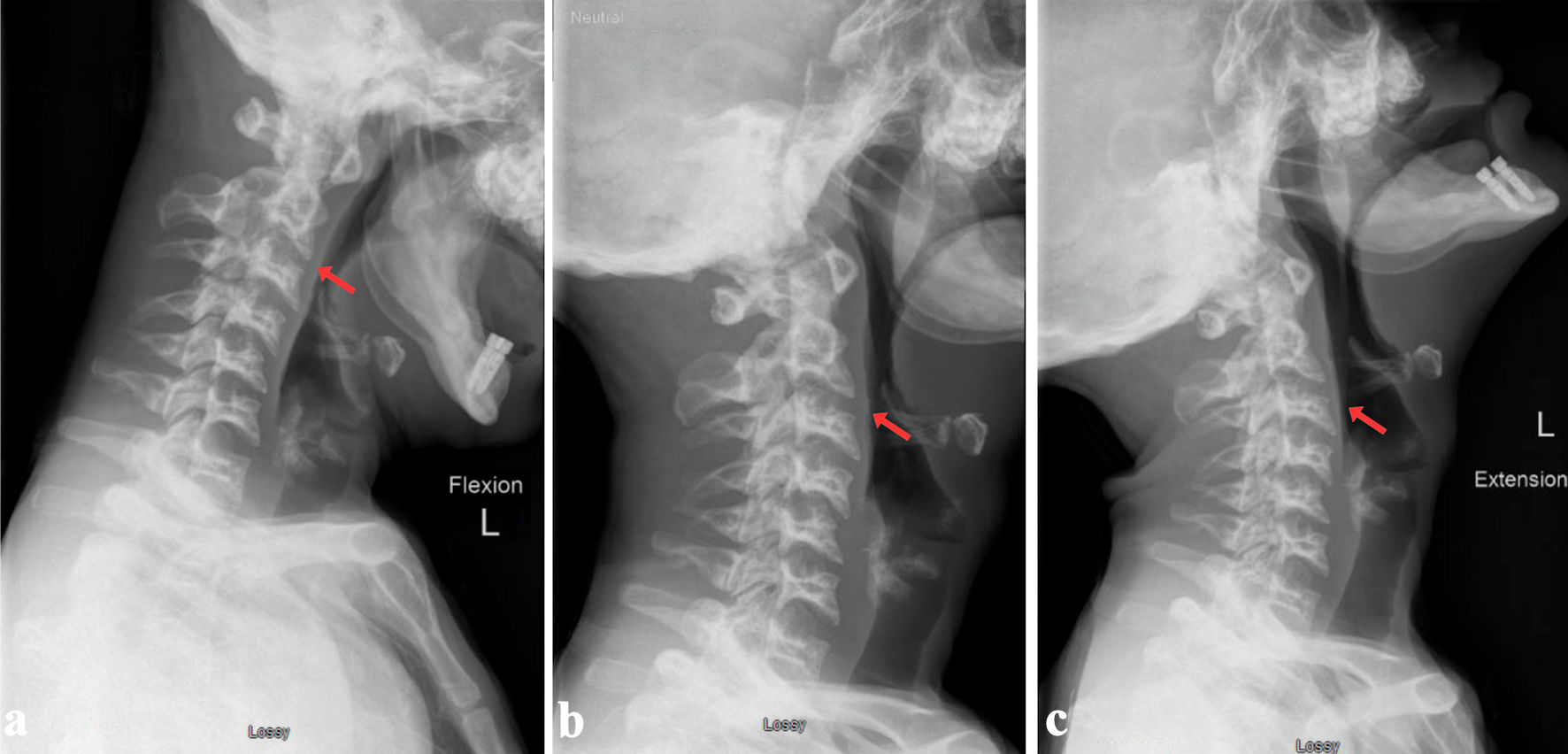
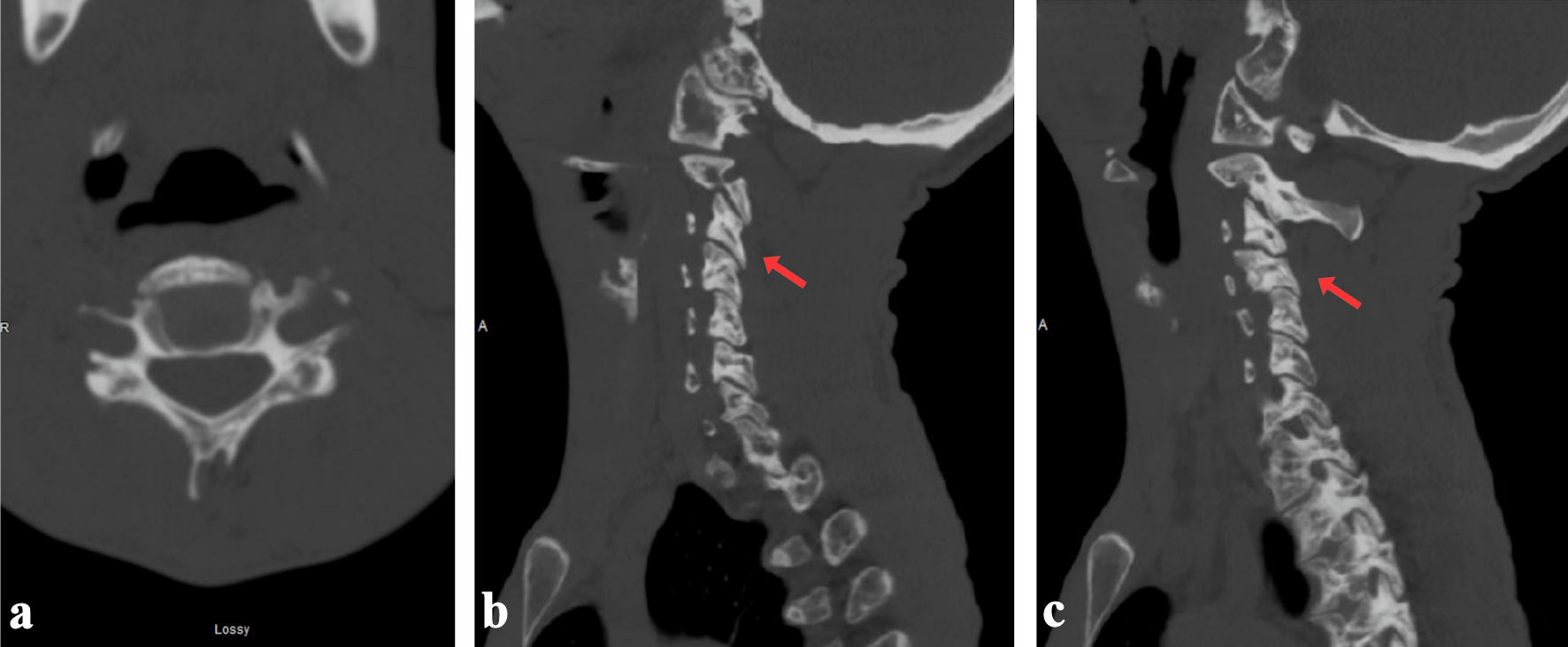
Immobilized in a rigid cervical orthosis (Miami J® collar)
and monitored with serial imaging. Three months post-injury, he remained asymptomatic with stable
cervical alignment. Dynamic flexion-extension CT of the cervical spine at 1 year post-injury showed
interval healing, with complete bone fusion of the C3 and C4 body fractures but incomplete fusion of
the C4 facet and lamina. |