Figures
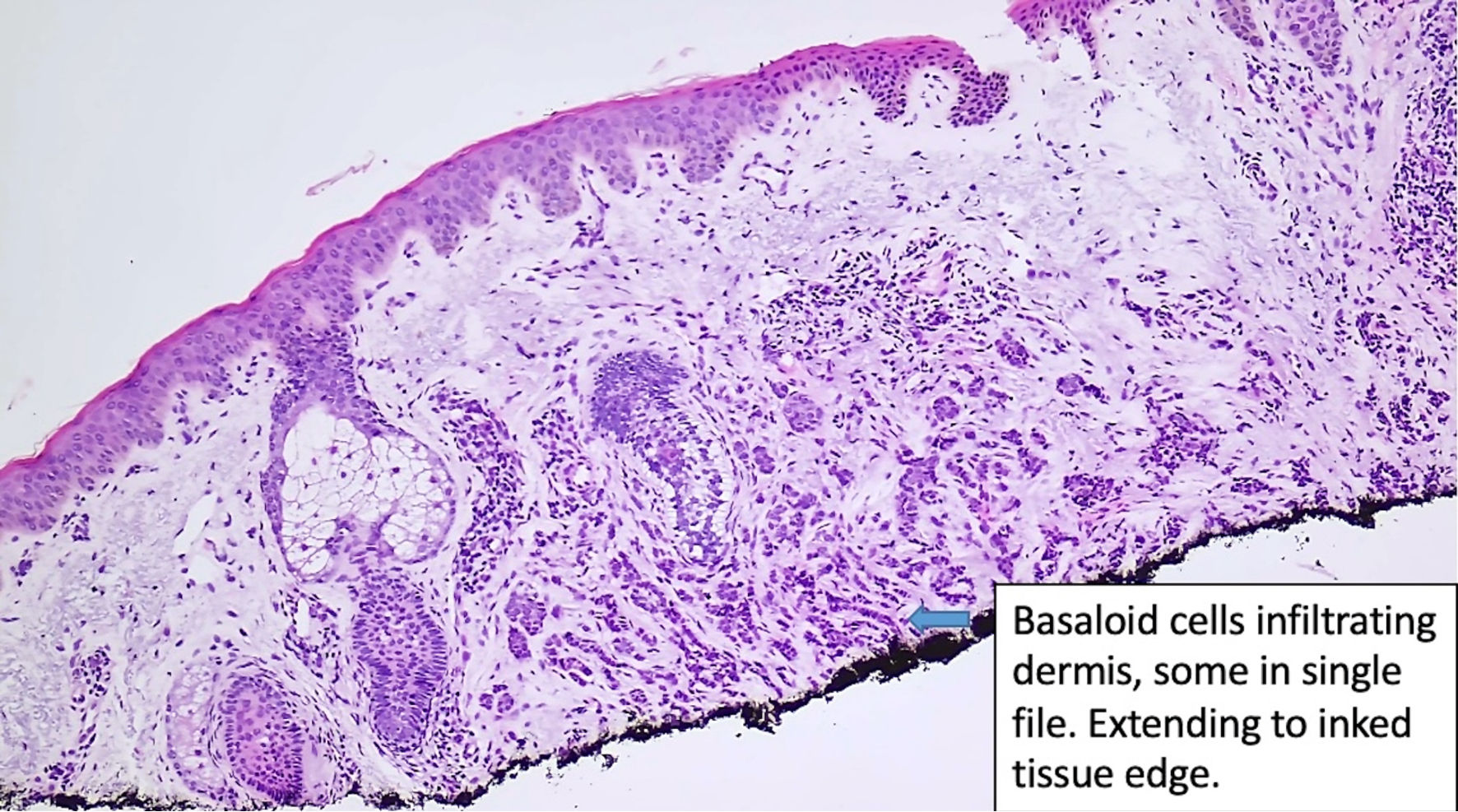
↓ Figure 1. Histologic features of eccrine
carcinoma at the initial diagnosis. Basaloid cells are infiltrating the dermis. (original magnification
× 100).
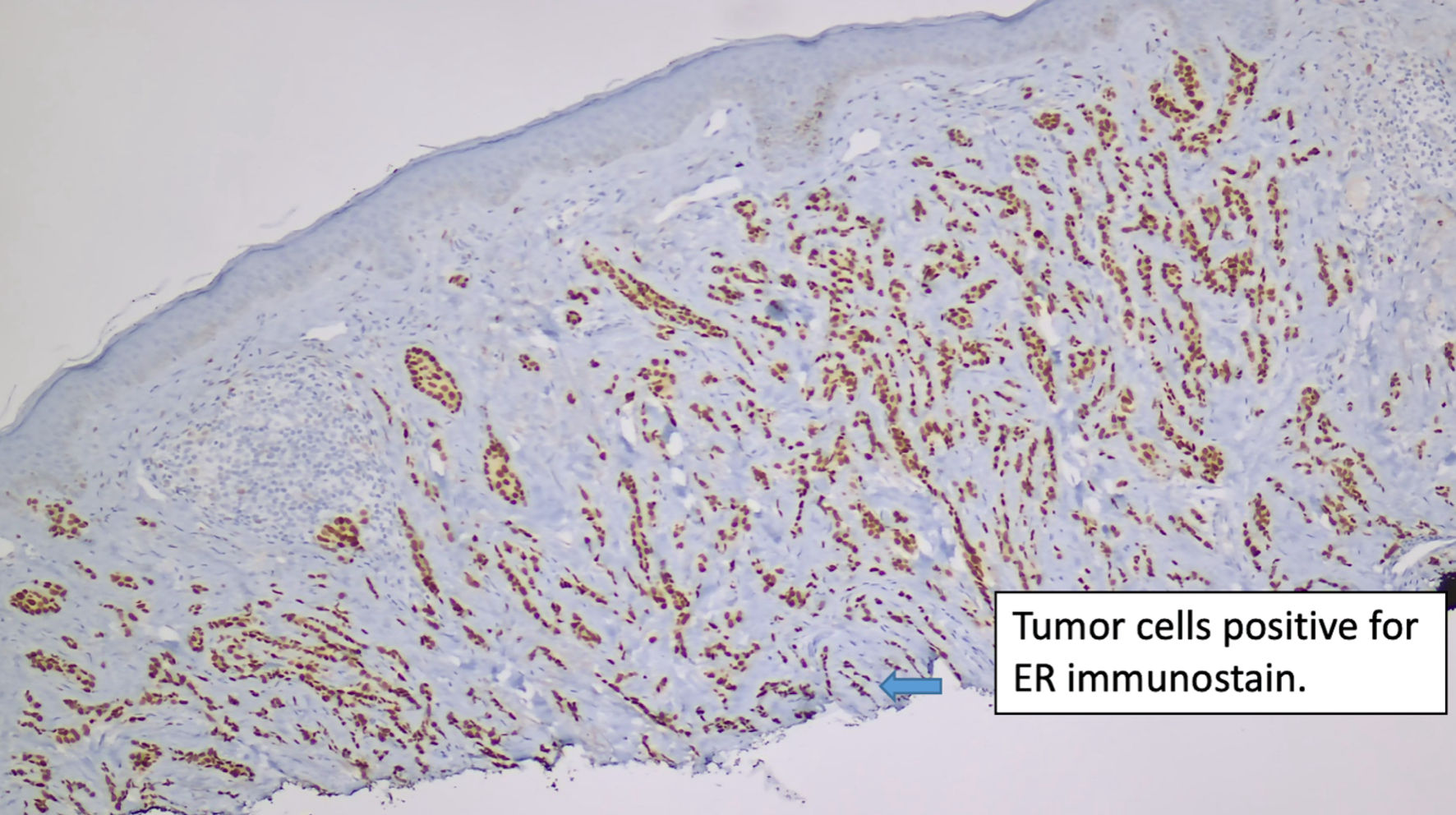
↓ Figure 2. Immunostain for ER (original
magnification × 100). ER: estrogen receptor.
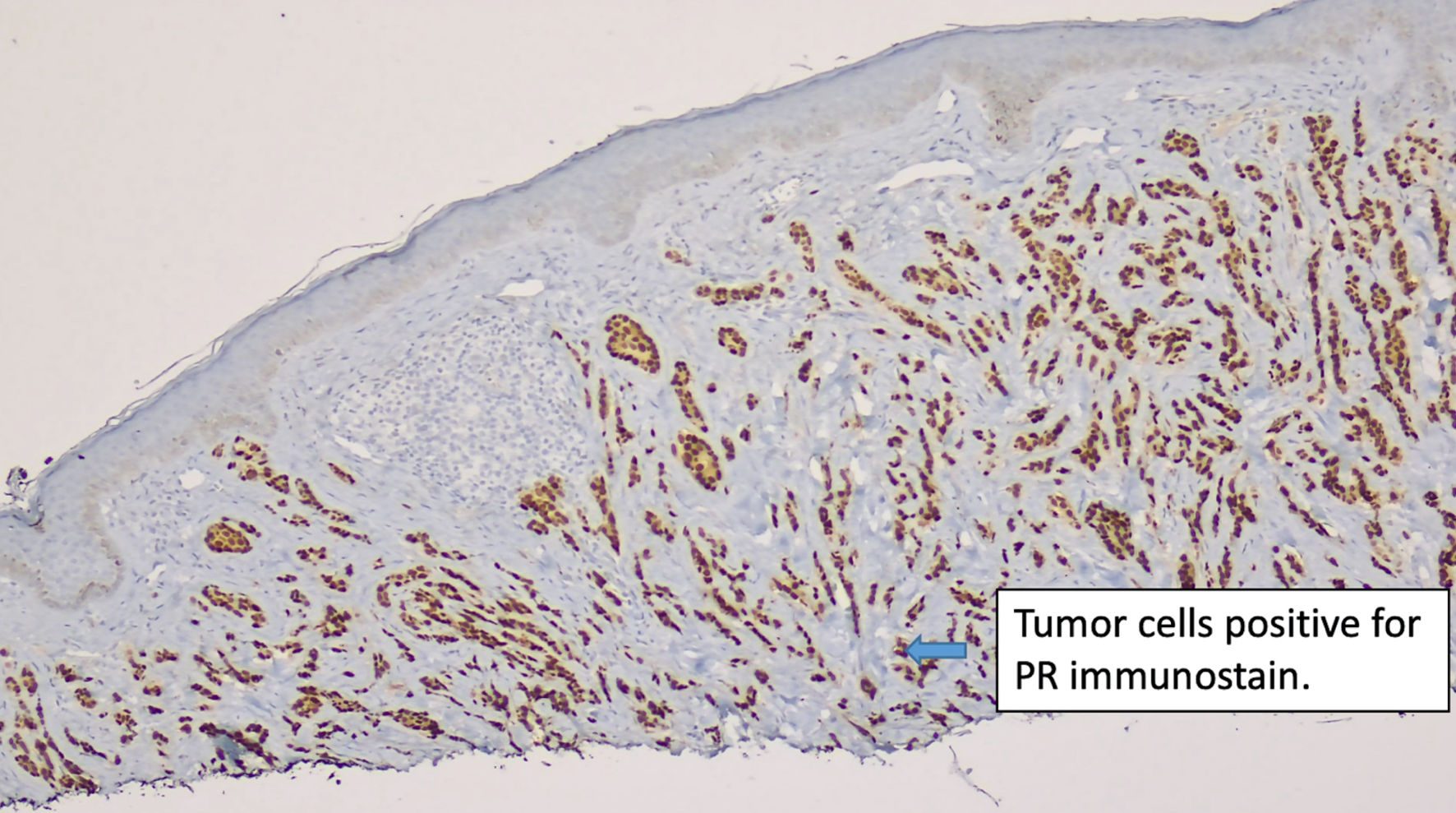
↓ Figure 3. Immunostain for PR (original
magnification × 100). PR: progesterone receptor.
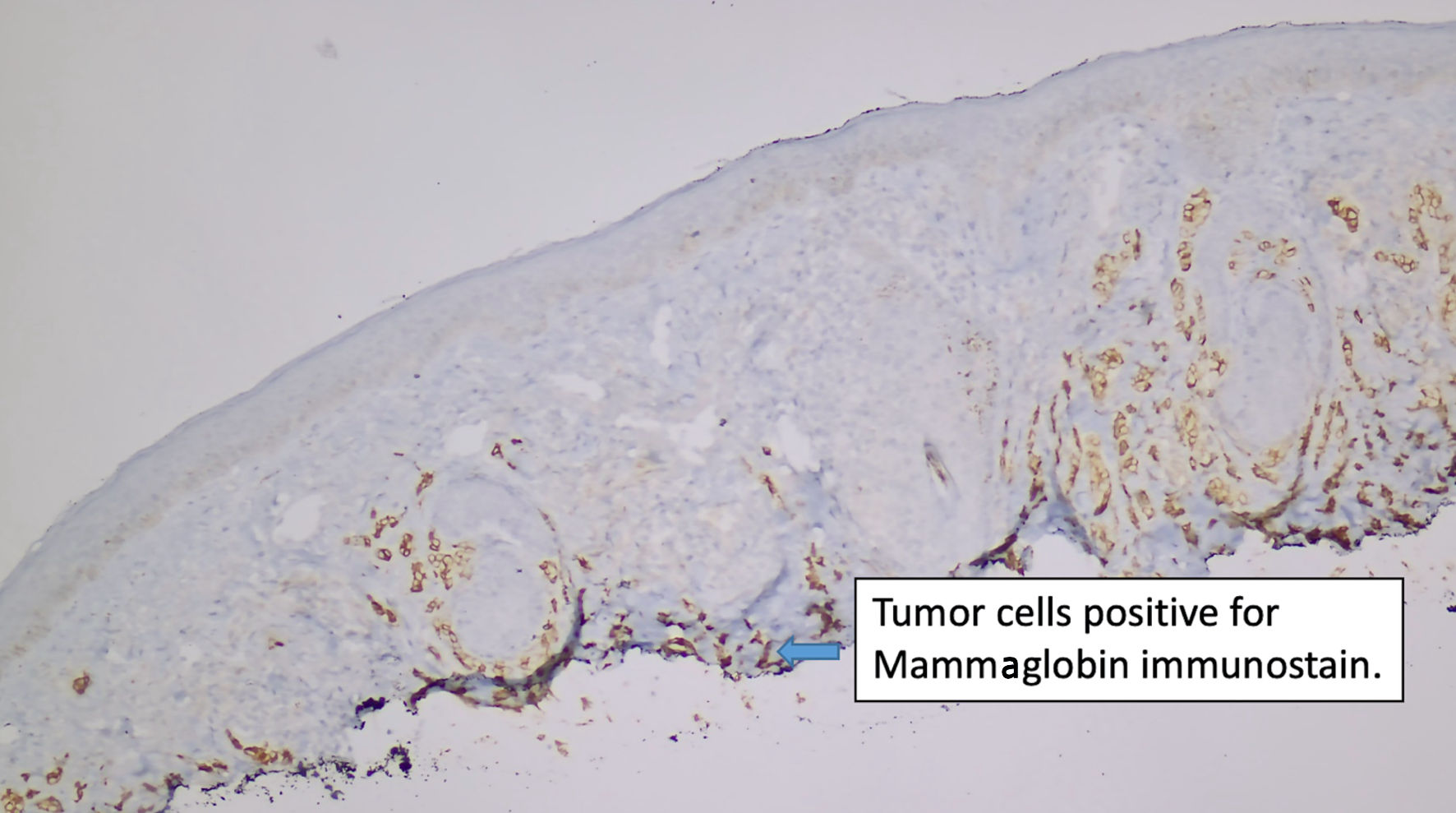
↓ Figure 4. Immunostain for mammaglobin (original
magnification × 100).
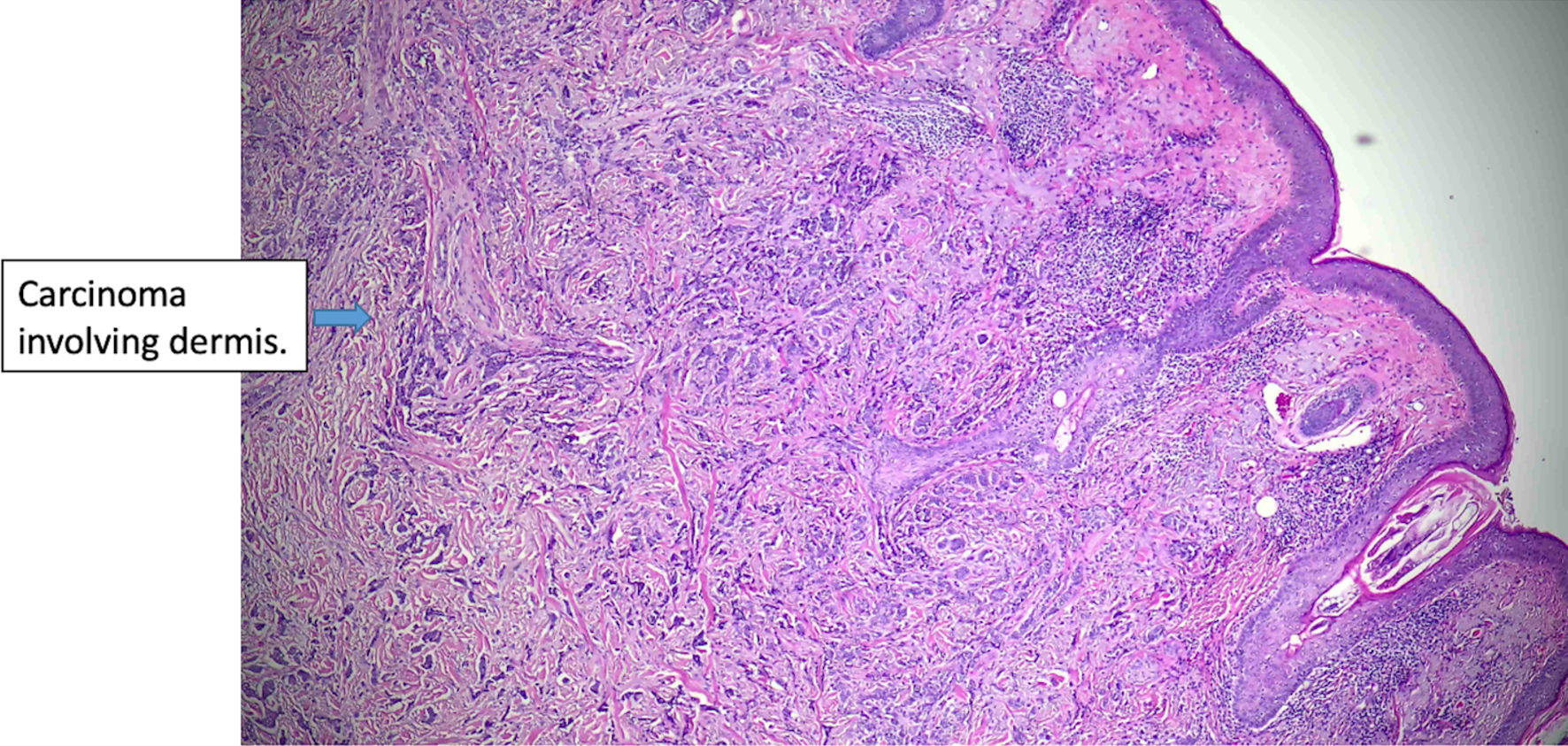
↓ Figure 5. Histologic features of eccrine cell
carcinoma at excision. The carcinoma is infiltrative, largely involving the dermis (original
magnification × 50).
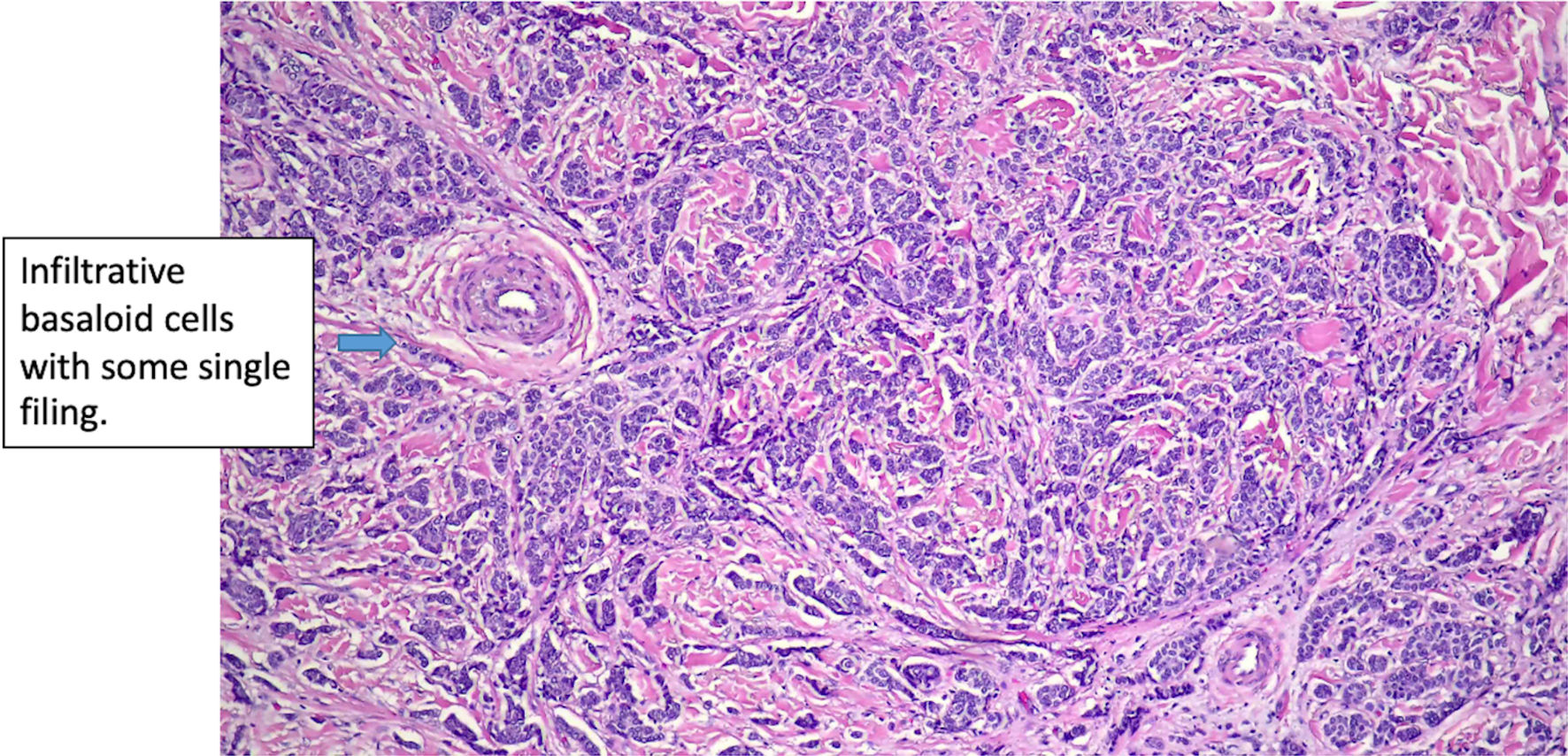
↓ Figure 6. Histologic features of eccrine cell
carcinoma at excision. (original magnification × 200).
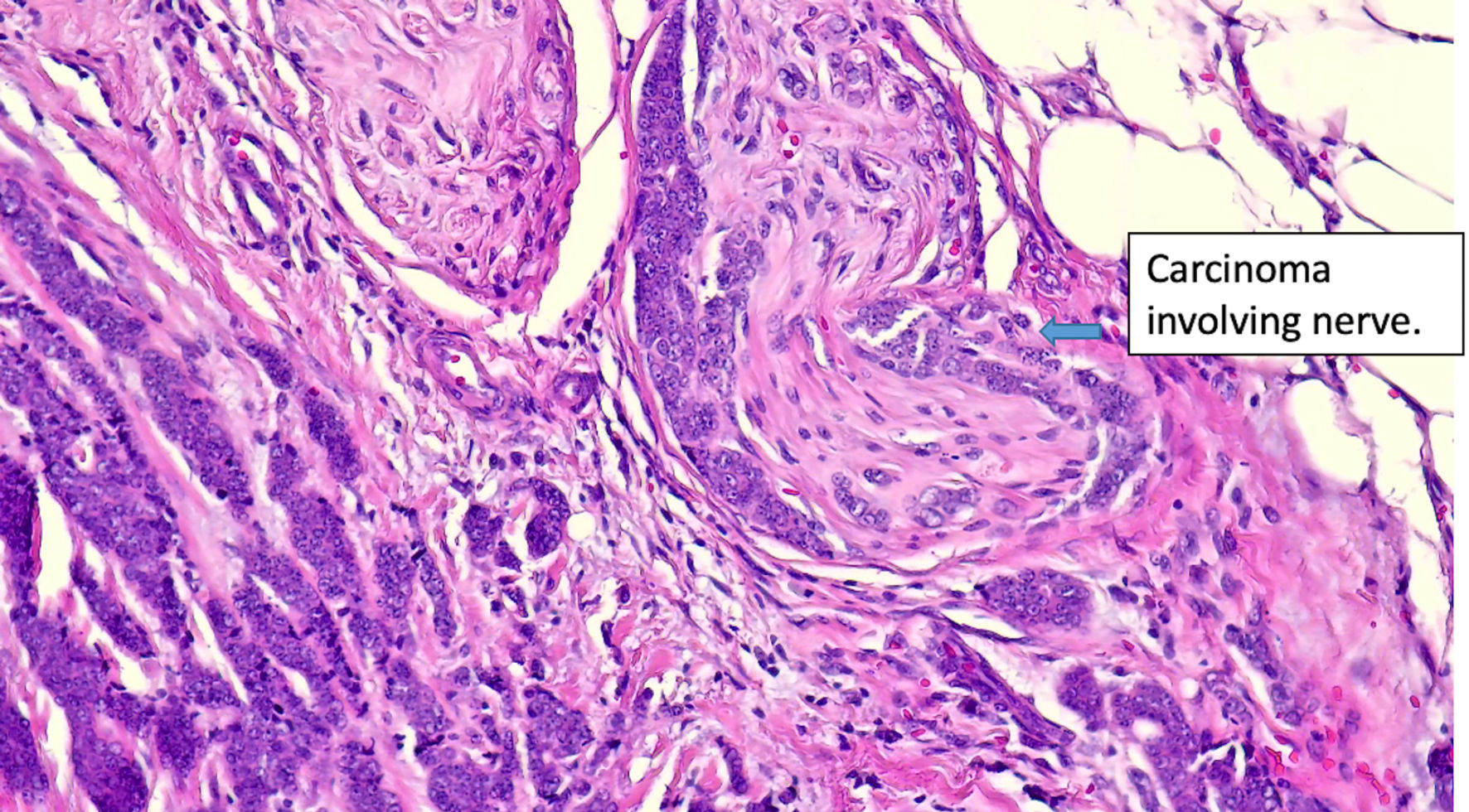
↓ Figure 7. Histologic features of eccrine cell
carcinoma at excision. Extensive perineural invasion. (original magnification × 400).
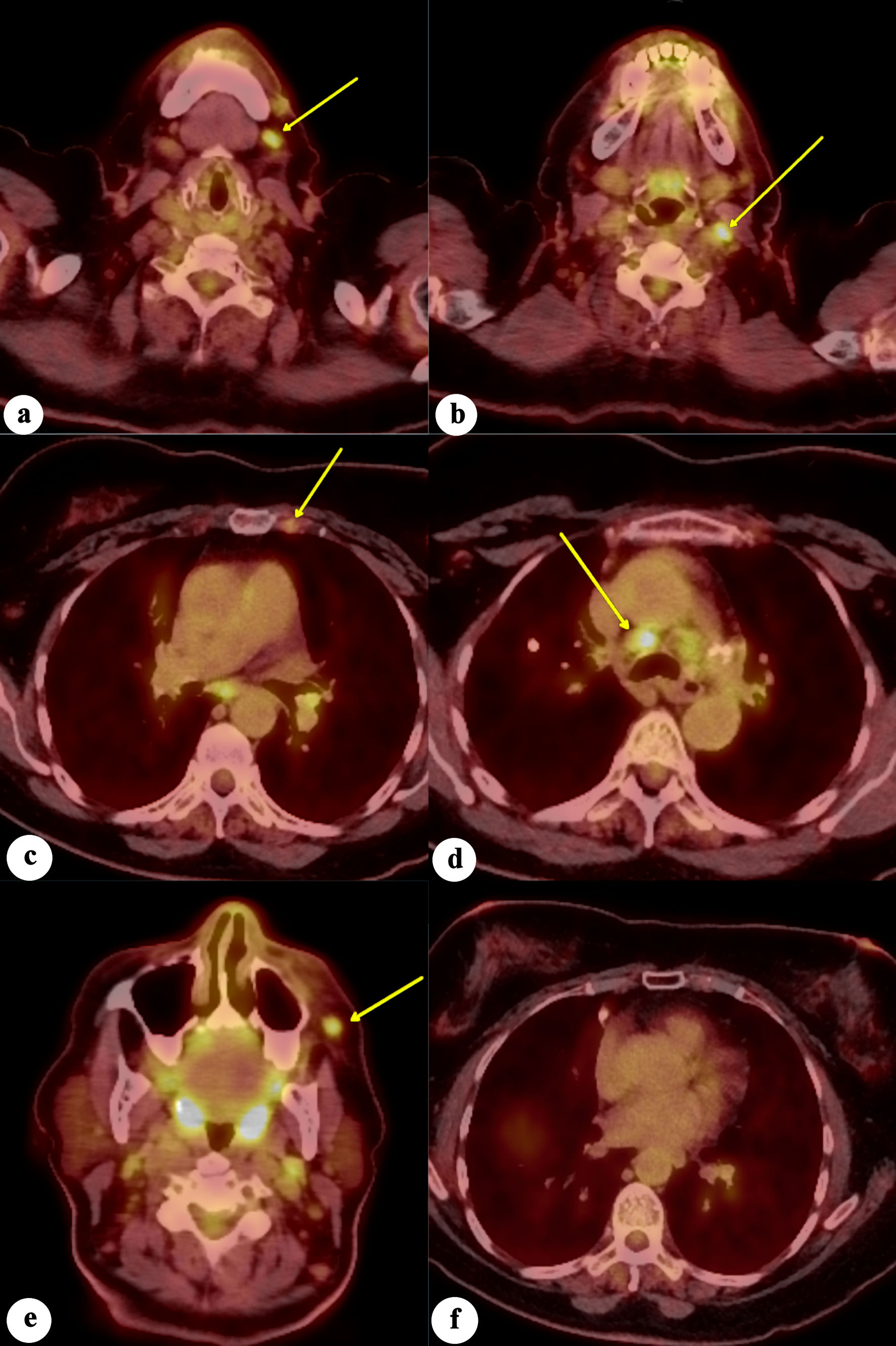
↓ Figure 8. Fluorodeoxyglucose positron emission
tomography/computed tomography (FDG-PET/CT) scan of the whole body demonstrates increased FDG avidity in
(a) left level 1 lymph node, (b) left level 2 lymph node, (c) left internal mammary lymph node, (d)
mediastinal/paratracheal lymph node, and (e) left malar soft-tissue nodule (yellow arrows), concerning
for metastatic disease. (f) No evidence of increased FDG avidity within the breast tissues to suggest
neoplastic disease.