| 30 M prior to initial presentation |
Deceased donor kidney transplant for ESRD (hypertensive nephrosclerosis).
|
Immunosuppression with tacrolimus, mycophenolate, prednisone. |
Stable graft function post-transplant. |
| 6 M prior to initial presentation |
Progressive abdominal discomfort, early satiety, unintentional weight
loss. |
Symptom monitoring. |
Worsening symptoms over months. |
| Initial presentation, “day 0” |
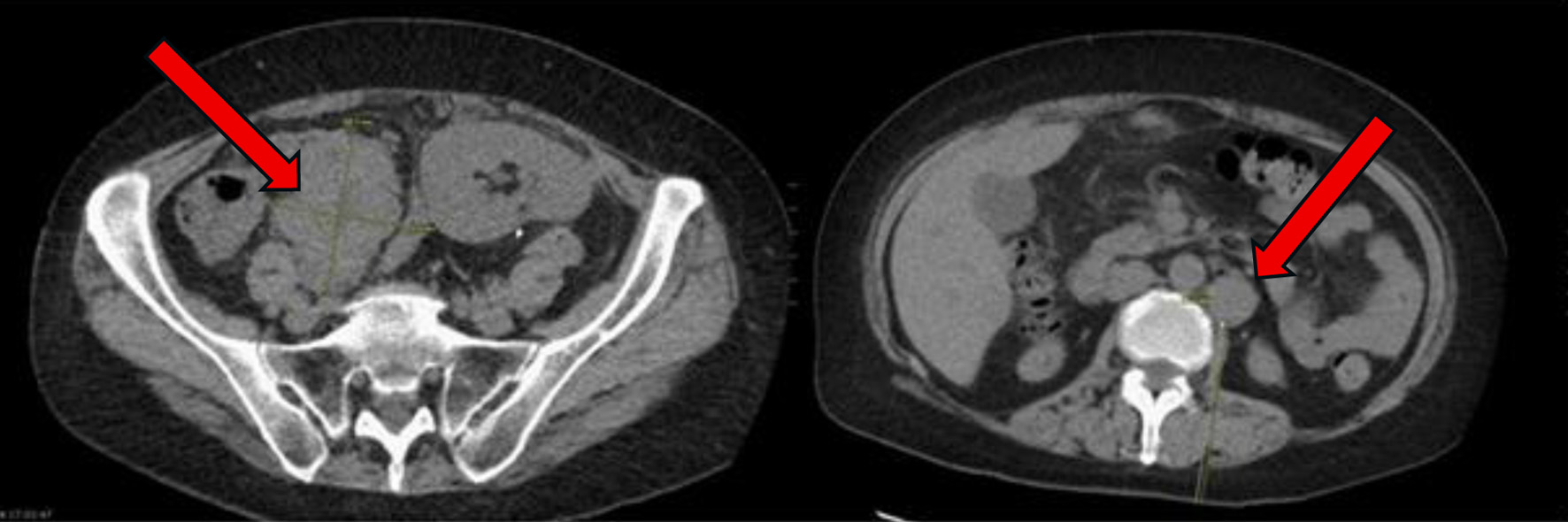
Abdominal pain and fatigue. CT abdomen and pelvis showing increase in size
of the abdominal and pelvic lymph nodes suspicious for post-transplant lymphoproliferative disorder
(Fig. 2). |
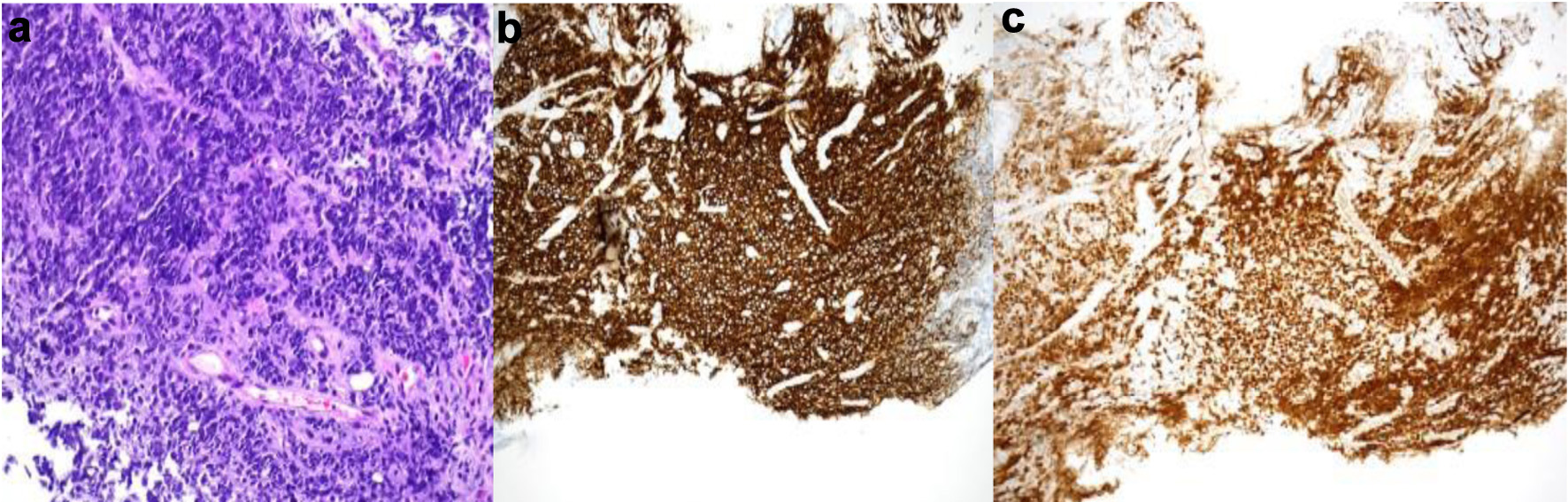
Retroperitoneal lymph node biopsy. |
Diagnosed with EBV-negative DLBCL, germinal center B-cell subtype PTLD.
|
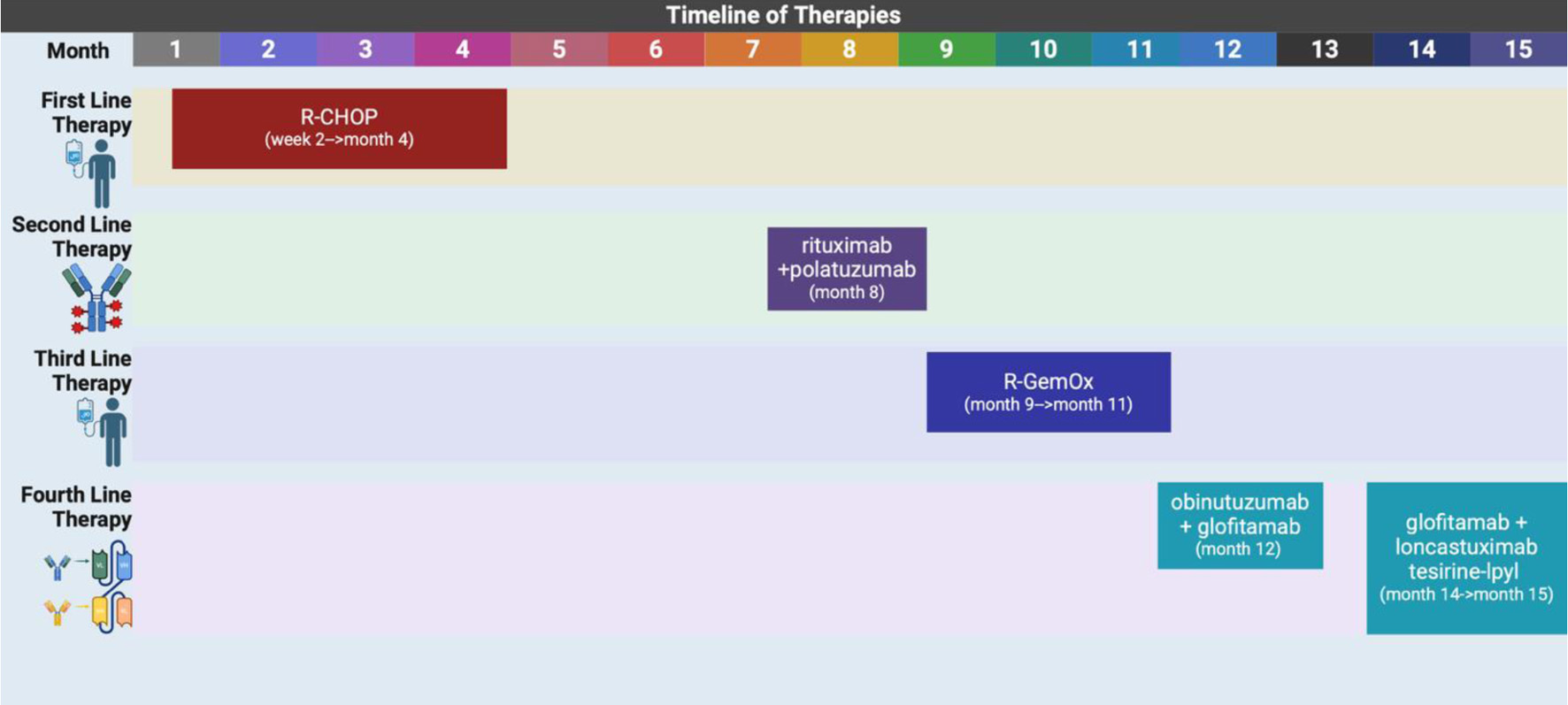
| 2 W after presentation |
Initiated first cycle of R-CHOP. |
Rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone. |
Mild neutropenia, partial radiographic response after two cycles. |
| 4 M after presentation |
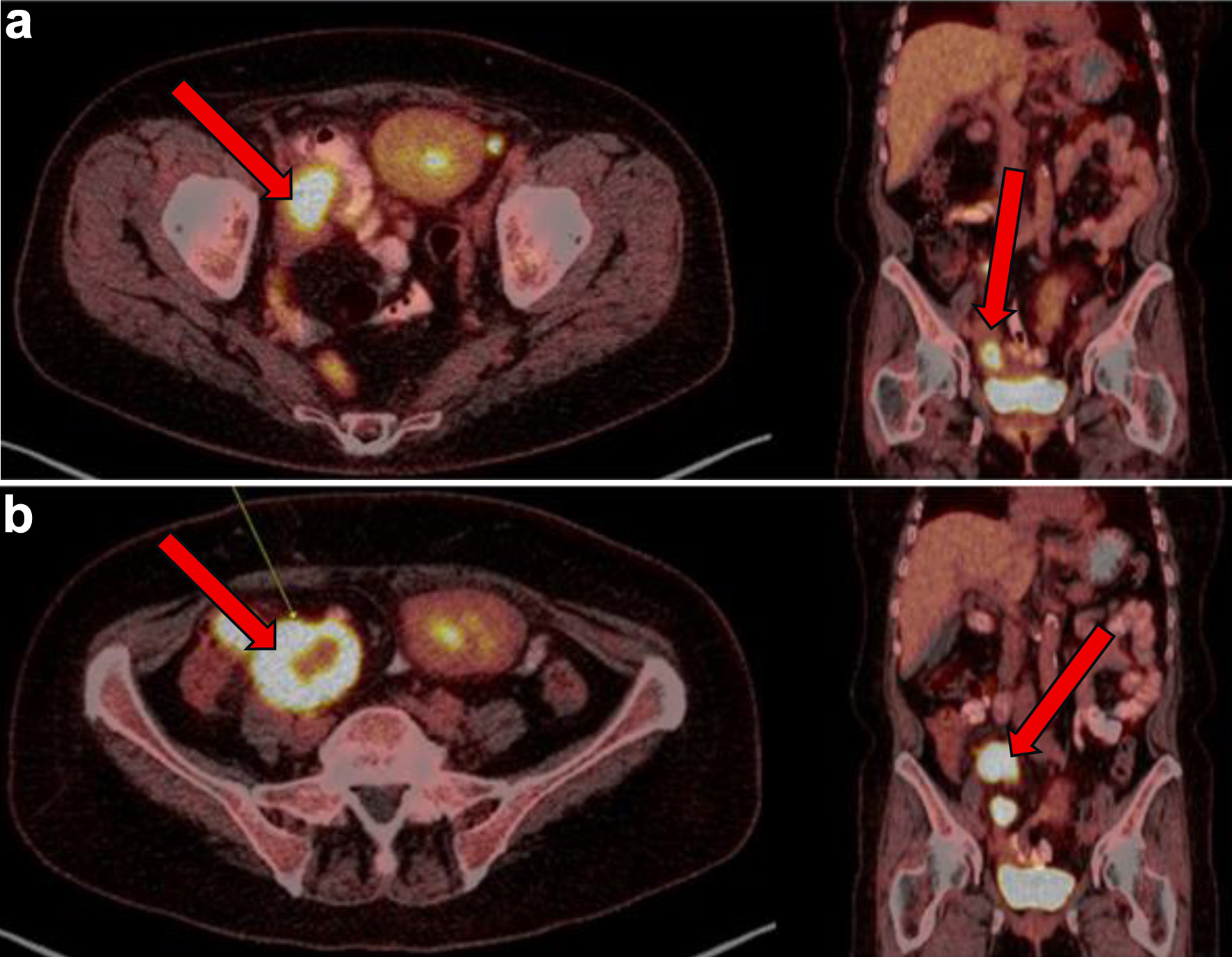
Disease progression post six cycles of R-CHOP. PET: new pelvic nodes,
bowel lesions (Fig. 3). |
Biopsy of right pelvic node: residual DLBCL with necrosis, high Ki-67, GC
phenotype. |
Confirmed refractory disease. |
| 8 M after presentation |
Started on rituximab + polatuzumab vedotin (delayed due to
hospitalizations). |
Chemotherapy initiated. |
Admitted to ICU with septic shock post-cycle. |
| 8 - 9 M after presentation |
EGD/colonoscopy: gastric ulcer (DLBCL), CMV colitis. |
Multidisciplinary discussion; suppressive antibiotics. |
Decision to continue therapy. |
| 9 - 11 M after presentation |
Four cycles of R-GemOx. |
Tolerated treatment initially. |
CT in October: disease progression with worsening abdominal pain. |
| 12 M after presentation |
Bridging therapy initiated: obinutuzumab + glofitamab for CAR T-cell
consideration. |
Admitted for CRS monitoring after first dose. |
Discharged, tolerated initial treatment. |
| 13 - 14 M after presentation |
Polatuzumab added. Recurrent admissions for GI toxicity (C.
difficile colitis, pain). |
Supportive care, pain control. |
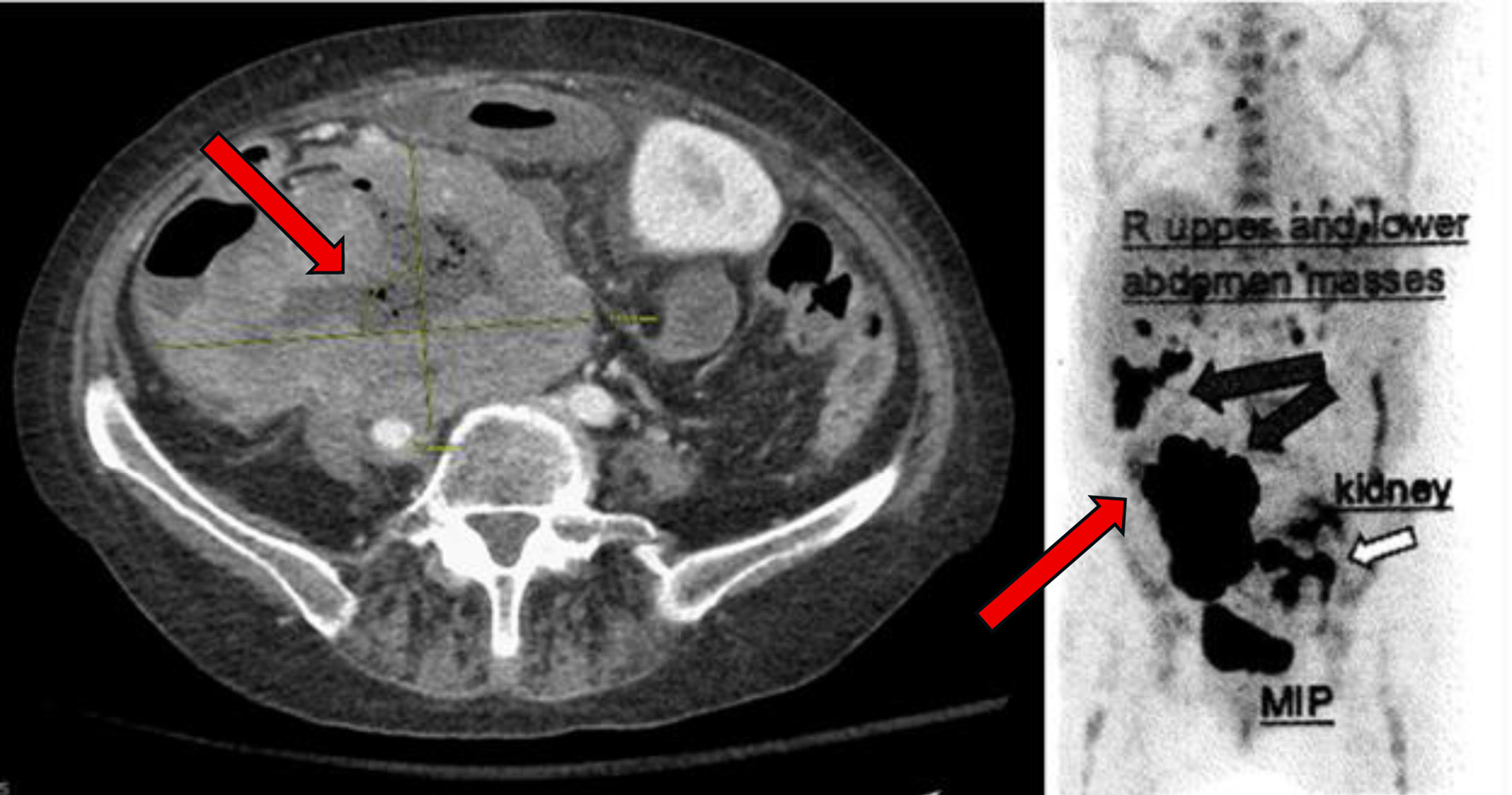
CT: tumor progression (up to 11.9 cm mass), new ascites. |
| 14 - 15 M after presentation |
PET scan confirms disease progression (Fig. 4). |
Started glofitamab + loncastuximab tesirine-lpyl (LOTIS-7 trial). |
Admitted soon after first dose with pain, fevers. |
| 15 M after presentation |
Emotional distress, ongoing symptoms. Imaging: no new disease. |
Goals-of-care discussion. Transitioned to hospice care. |
Patient chose to stop treatment. |