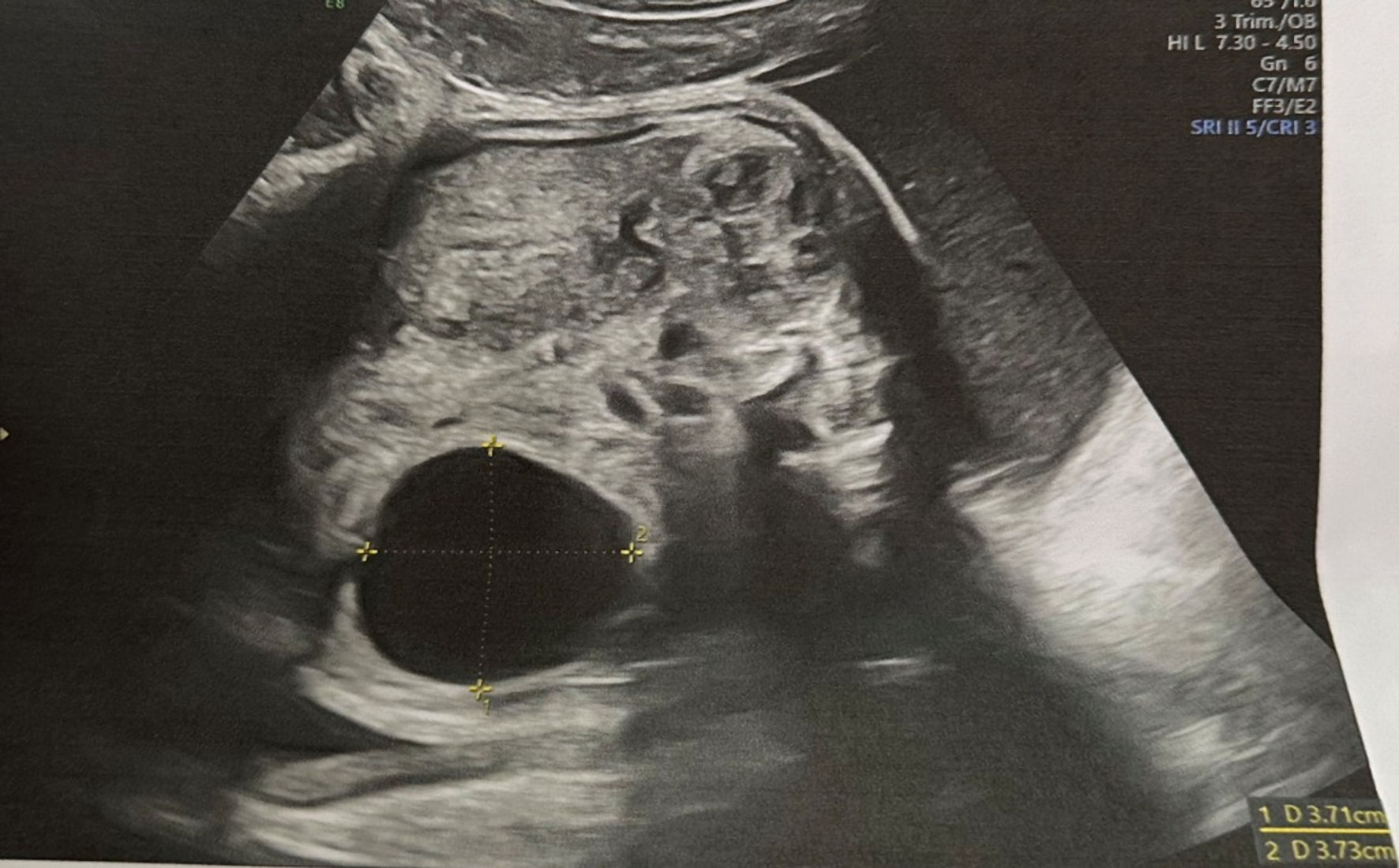
↓ Figure 1. Simple thin-walled cystic formation
localized separately from kidney seen in 27th week of gestation.
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://jmc.elmerpub.com |
Case Report
Volume 16, Number 10, October 2025, pages 415-420
Fetal Ovarian Cysts in Prenatal Imaging: Diagnostic Challenges and Management Options
Figure
Table
| Type | Sonographic features |
|---|---|
| Choledochal cyst | Localized in the right upper quadrant behind the portal vein, connected with the bile ducts and gallbladder; increase in size with increasing gestational age [17] |
| Intestinal duplication cyst | Round/oval shaped mass, closely associated with the intestinal tract; possible compression of the adjacent intestine resulting in intestinal obstruction and polyhydramnios [17] |
| Duodenal atresia | “Double-bubble sign” [18] |
| Mesenteric cyst | Typically anechoic, thin-walled, possible internal septi, movable with peristalsis [19] |
| Urachal cyst | Anechoic cyst at the base of umbilical cord, connected to urinary bladder, surrounded by umbilical arteries [20] |
| Abdominal lymphangioma | Multiseptated, multicystic irregular mass with rapid grow; association with other abnormalities - skin edema, hydrops fetalis, polyhydramnios [21] |
| Hydrometrocolpos | Мidline, cystic, pear-shaped pelvic mass, often located posterior to the bladder; bilateral hydronephrosis may also be present due to urinary tract obstruction [22] |