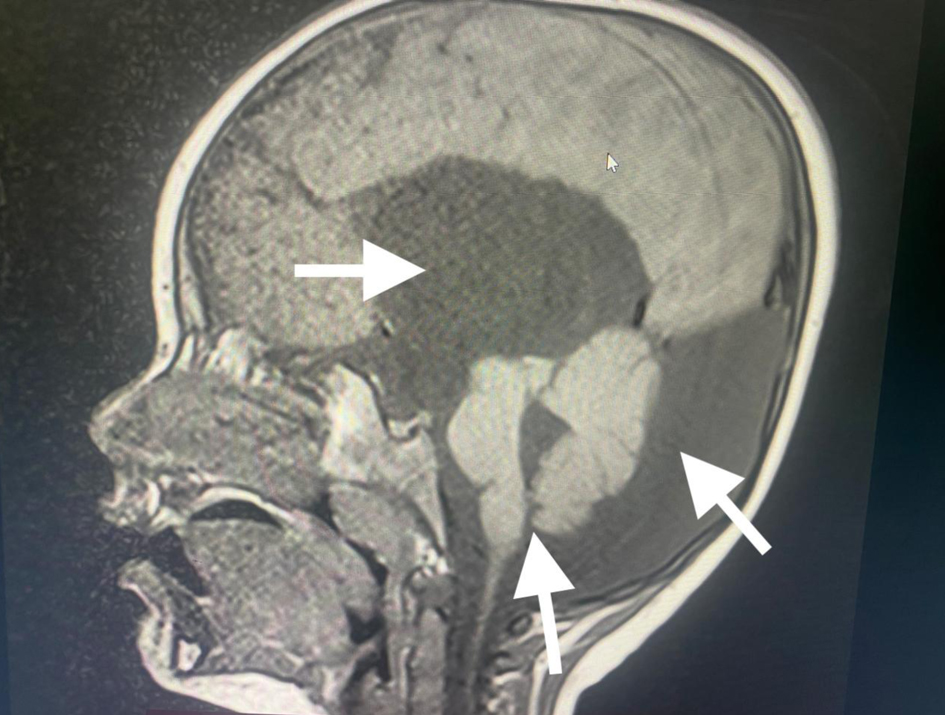
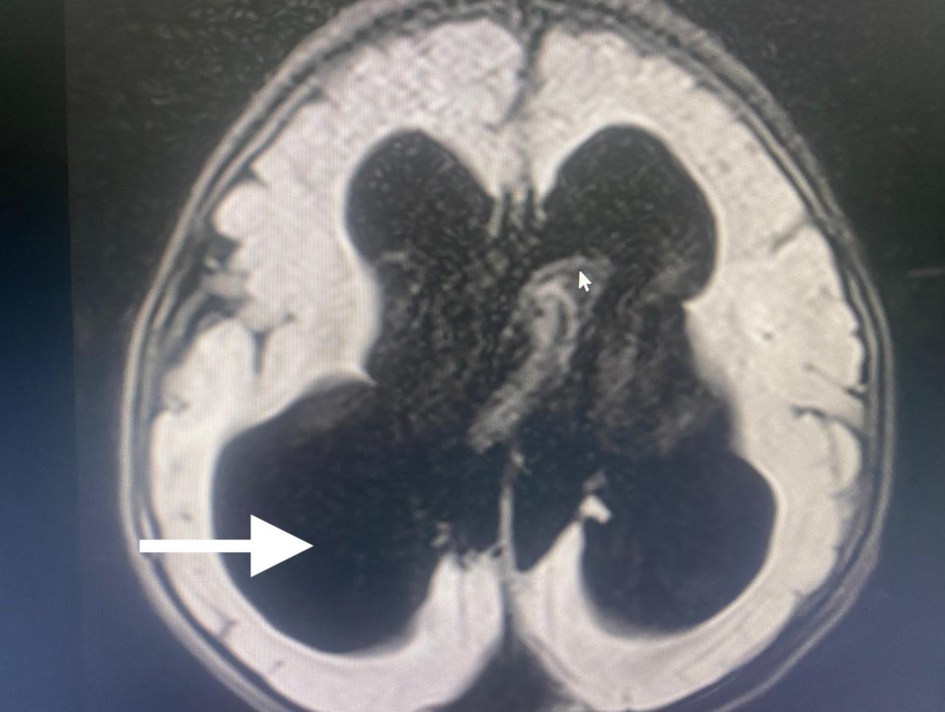
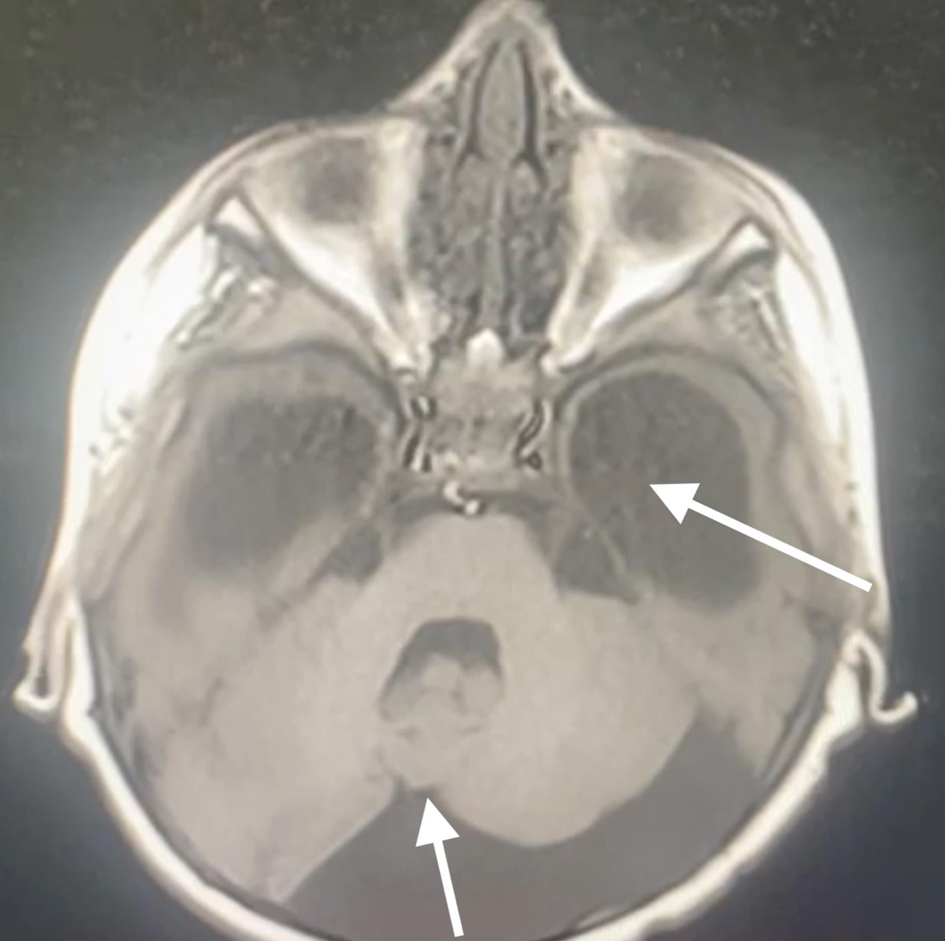
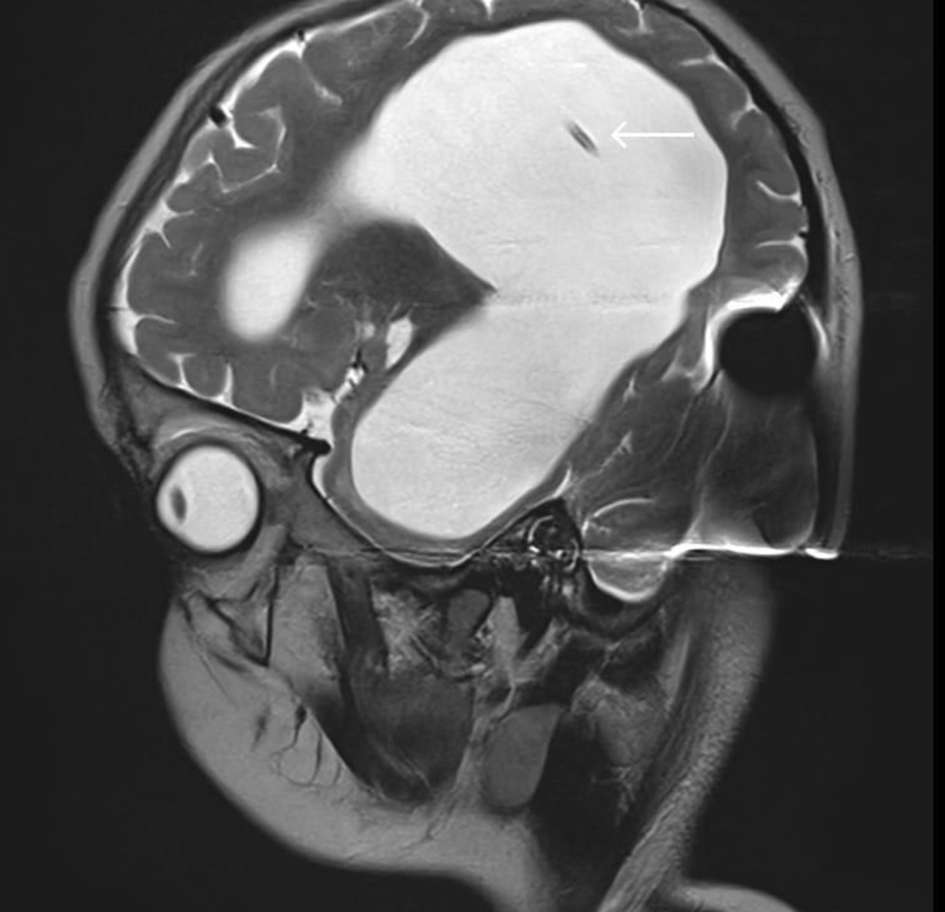
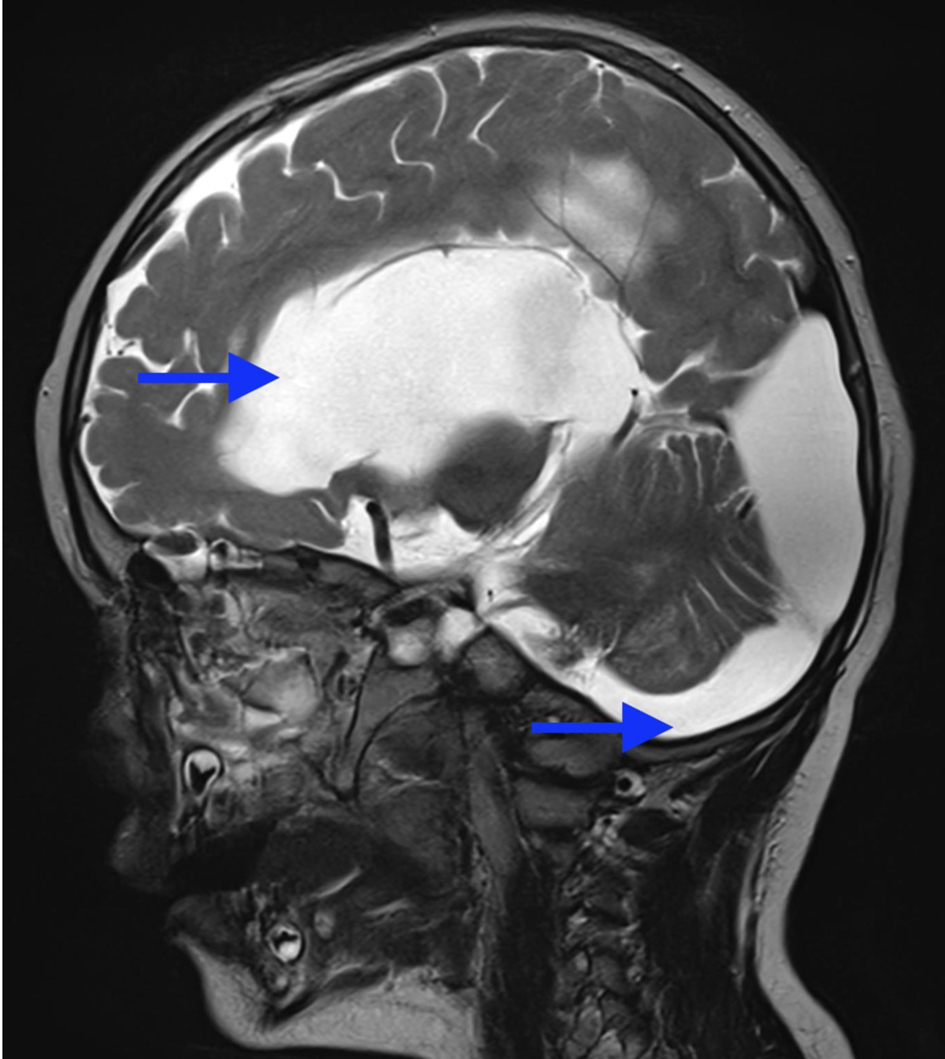
↓ Figure 1. Preoperative head MRI demonstrating
agenesis of the cerebellar vermis, dilatation of the fourth ventricle, and hydrocephalus (arrows). MRI:
magnetic resonance imaging.
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://jmc.elmerpub.com |
Case Report
Volume 16, Number 9, September 2025, pages 337-344
Anesthesiologist’s Concerns About Dandy-Walker Syndrome: Airway Management, Muscle Relaxants, and Train-of-Four Monitoring of Neuromuscular Blockade
Figures




Table
| Situation | Management considerations | Recommended actions |
|---|---|---|
| Pediatric neuroanesthesia expertise | Requires specialized pediatric and neuroanesthetic skills | Fellowship or extended training programs for advanced experience |
| Airway management | 1) Macrocephaly, micrognathia, macroglossia; 2) Cervical spine anomalies; 3) Limited cooperation in pediatric patients. |
1) Thorough preoperative airway assessment; 2) Difficult airway protocol in place; 3) Consider laryngeal mask airway or video laryngoscope if conventional intubation fails. |
| Intubation | High risk of failed conventional intubation | 1) Prepare alternative devices; 2) Ensure rapid, atraumatic intubation |
| Anesthetic technique | 1) Risk of postoperative respiratory complications; 2) Brainstem dysfunction. |
1) Total intravenous anesthesia with short-acting agents; 2) Avoid muscle relaxants if train-of-four monitoring unavailable; 3) Ensure rapid emergence. |
| Postoperative respiratory care | Risk of apnea, aspiration, atelectasis, prolonged ventilation | 1) Close monitoring in postanesthesia care unit; 2) Respiratory exercises as indicated; 3) Train-of-four monitoring if muscle relaxants used. |
| Pain management | Limitations due to respiratory depression and bleeding risk | 1) Multimodal analgesia (nonsteroidal anti-inflammatory drugs,
paracetamol, ketamine, dexmedetomidine, regional techniques); 2) Reserve opioids for insufficient pain control. |
| Cardiac and other congenital anomalies | Possible coexisting defects | Comprehensive preoperative evaluation including electrocardiography and echocardiography |