| R-factor |
Classify type of liver injury (hepatocellular vs. cholestatic vs. mixed)
|
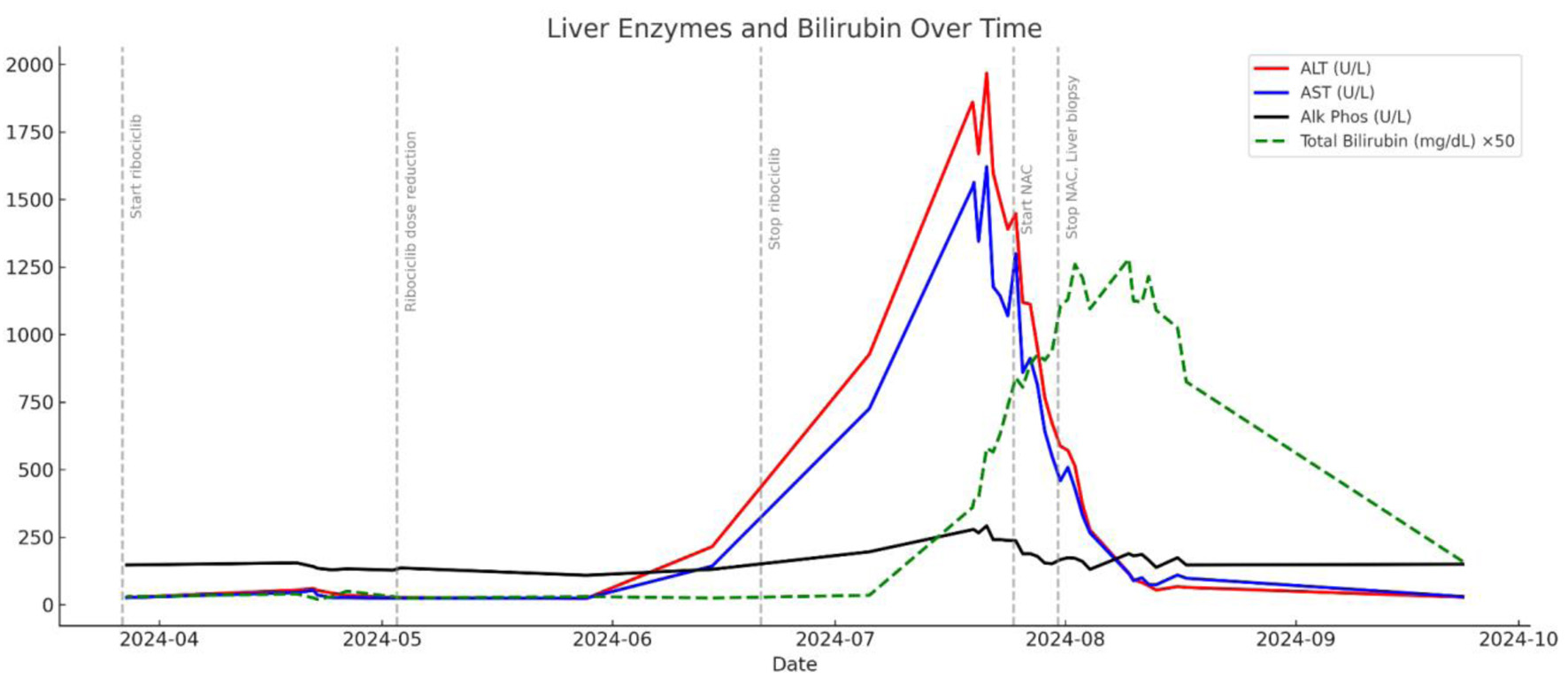
R = (ALT ÷ ALT ULN) ÷ (ALP ÷ ALP ULN); ALT = 1,825 U/L (ULN
= 40), ALP = 278 U/L (ULN = 120) |
R = (1,825/40) ÷ (278/120) = 20.73 |
Hepatocellular injury (R ≥ 5) |
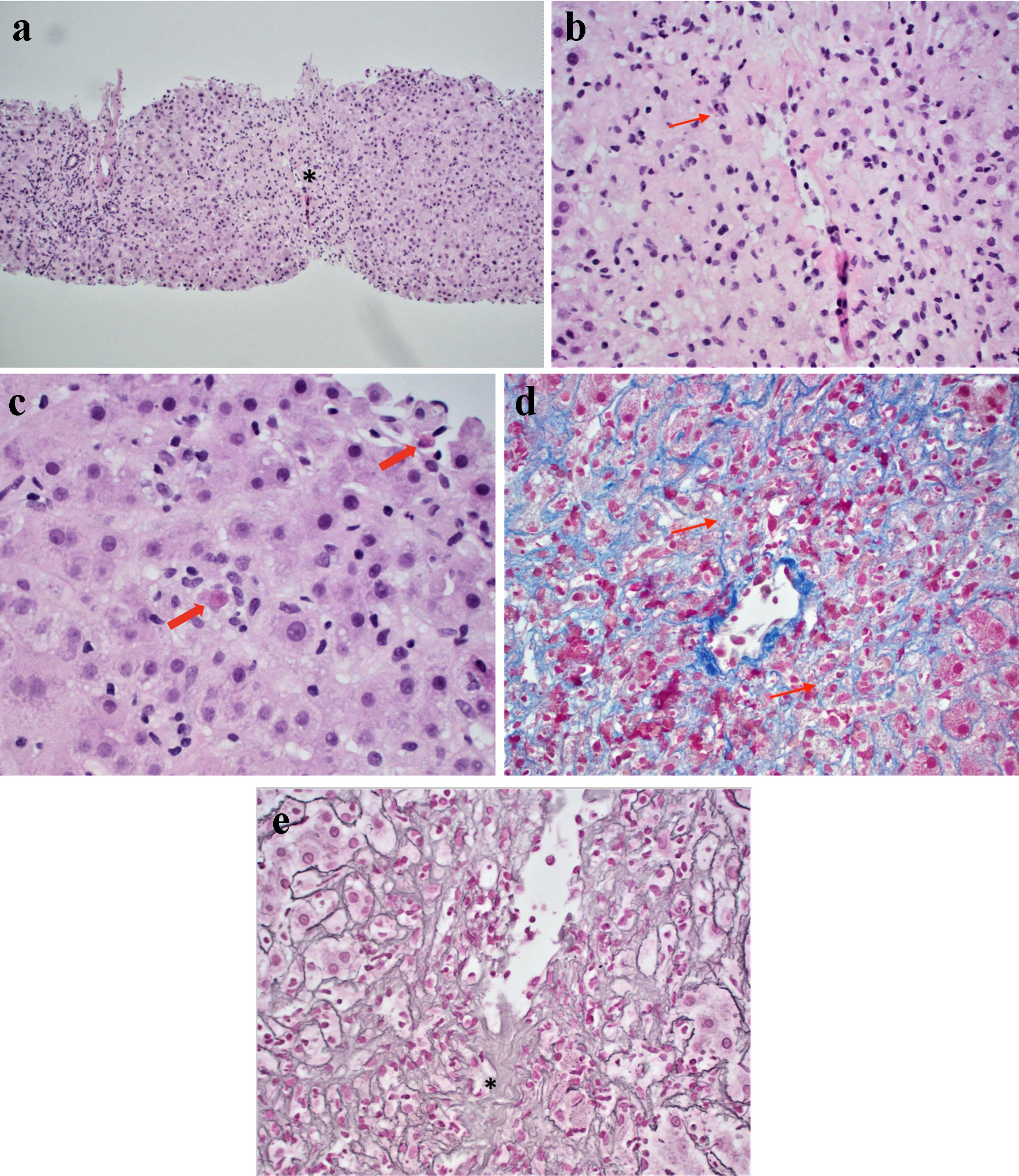
Confirms hepatocellular pattern, consistent with biopsy findings |
| RUCAM score |
Estimate likelihood of drug causality in DILI |
Temporal relationship, risk factors, exclusion of alternative causes,
dechallenge, known hepatotoxicity, rechallenge |
Components (approx): +2 (onset); +3 (dechallenge); +2 (no alt causes); +2
(known hepatotoxin); +1 (female); Total: ∼ 10 |
Highly probable (≥ 9) |
Strongly supports ribociclib as cause of liver injury |
| Naranjo algorithm |
General tool to estimate probability of ADR |
Includes timing, prior reports, dechallenge, rechallenge, alternative
causes |
Components (approx): +2 (timing); +1 (dechallenge); +1 (prior reports); +2
(no alt cause); +1 (biopsy); Total: ∼ 7 |
Probable ADR (5 - 8) |
Supports ribociclib as likely cause of DILI |