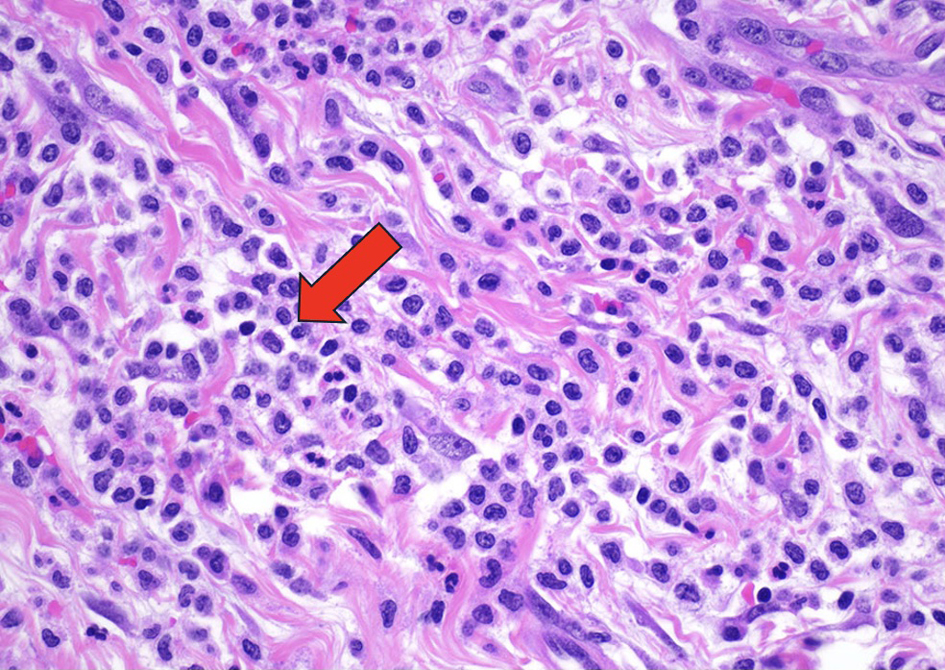
↓ Figure 1. The myocardium and surrounding
adipose tissue are architecturally effaced by an infiltrating lesion composed of immature mononuclear
cells demonstrating fine chromatin. Hematoxylin and eosin (H&E)-stained sections of the pericardium
demonstrated fibrovascular and fibroadipose tissue with a variably dense infiltration of medium sized
cells with irregular nuclear membranes, conspicuous nucleoli, and variable amounts of clear cytoplasm,
consistent with atypical/immature monocytic cells. These atypical cells formed diffuse sheets in some
areas and were seen with large numbers of mature granulocytes in other areas. The immature cells
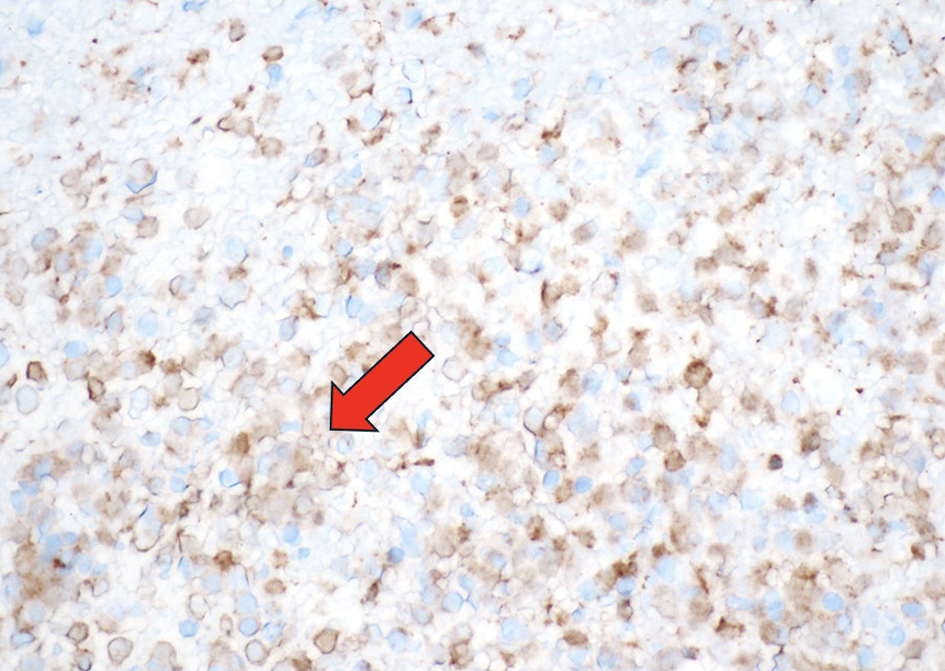
demonstrated positive staining for CD45, CD43, CD34, CD68, and CD163. They were negative for CD117, TdT,
CD3, CD20, CD56, calretinin, and WT1. The Ki-67 proliferation index was variably elevated. This atypical
monocytic infiltration is diagnostic of myeloid sarcoma (H&E, × 400). Arrow indicating immature
mononuclear cells infiltrating the cardiac tissue.