Figures
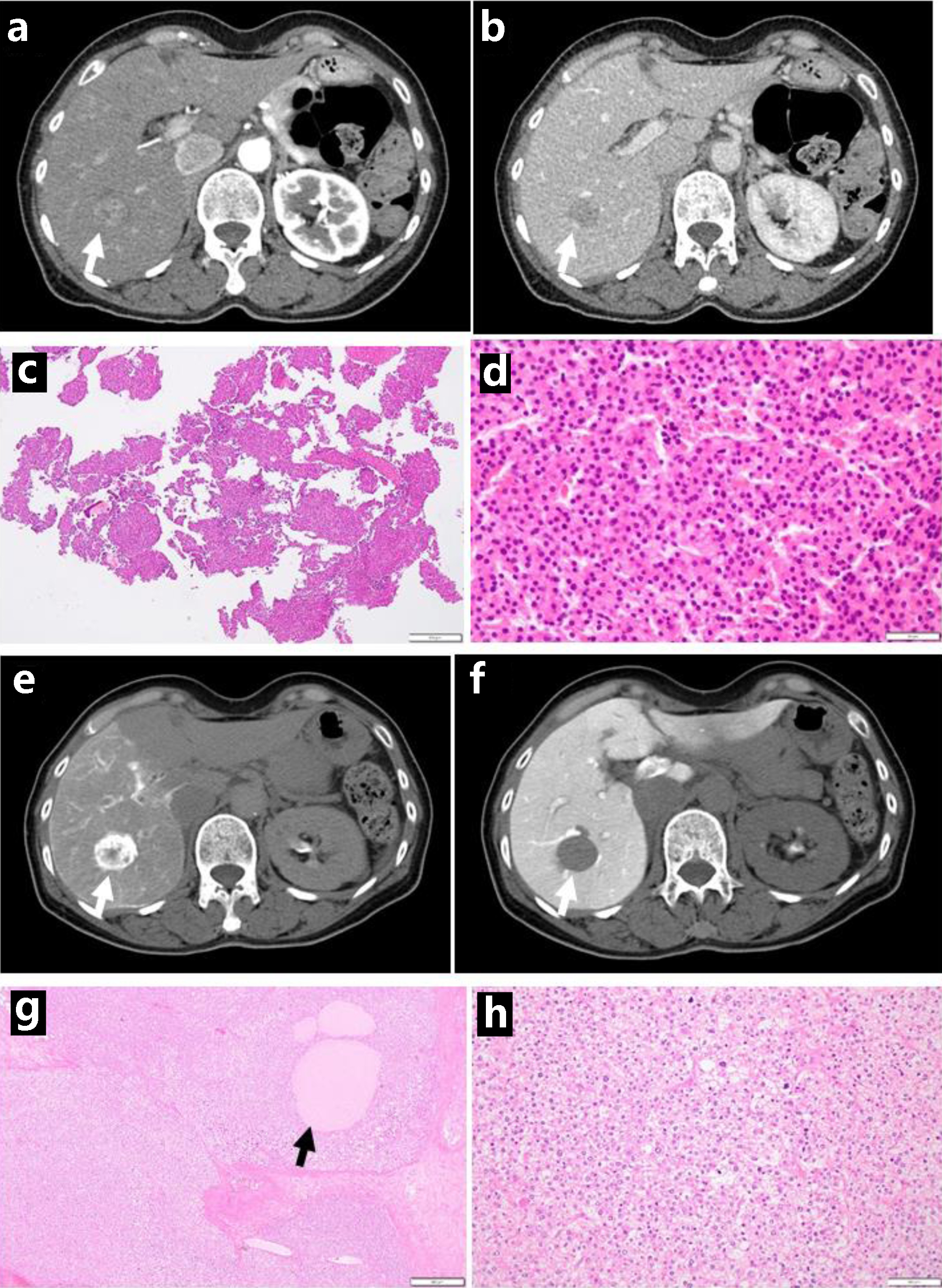
↓ Figure 1. Dynamic-enhanced computed tomography
scans with enhancement at the initial visit, showing early-phase enhancement (arrow, a) and late-phase
washout (arrow, b). Needle liver biopsy, showing hepatocellular carcinoma (c in low magnification, d in
high magnification). Computed tomography during hepatic arteriography with marked staining (arrow, e),
in contrast with computed tomography during arterial portography with no staining (arrow, f), consistent
with hepatocellular carcinoma. Note foamy cells with degeneration (h) and necrotic cell debris spaces
(arrow, g) after transcatheter arterial chemoembolization, compared with viable tumor cells (d). Scale
bar = 500 µm in c and g, 50 µm in d and h.
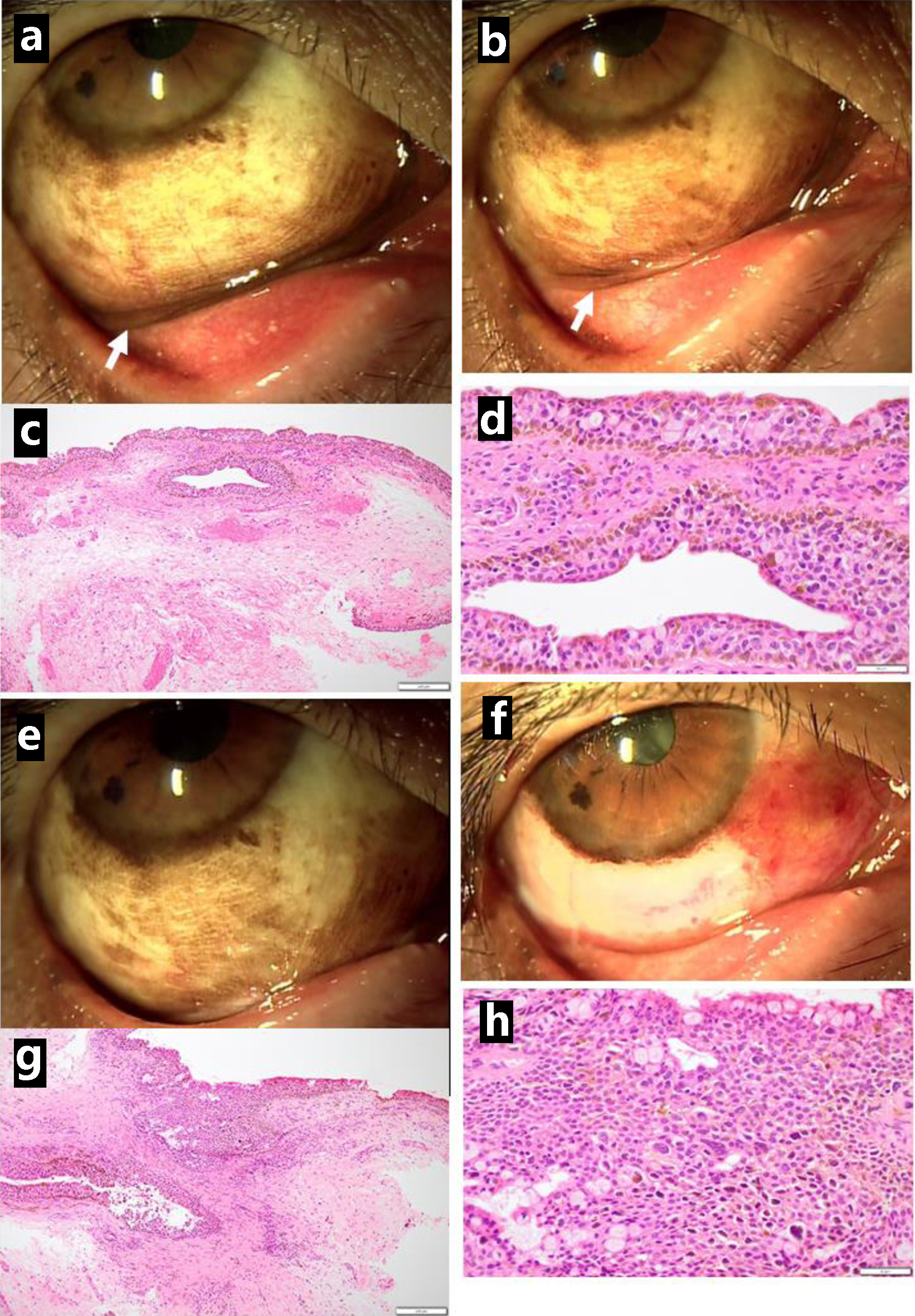
↓ Figure 2. Pigmented lesions mainly along the
lower conjunctival fornix (arrow, a) in the right eye just before excisional biopsy at the initial visit
and reduced pigmented lesions in the fornix (arrow, b) one month later. Excisional biopsy showing
conjunctival malignant melanoma in situ (c in low magnification, d in high magnification). Three
months after the initial visit, the lower bulbar conjunctiva excised as wide as possible (presurgical
photo in e, postsurgical photo in f). The excised tissue diagnosed as conjunctival malignant melanoma
in situ (g in low magnification, h in high magnification). Scale bar = 200 µm in c and g, 50
µm in d and h.
↓ Figure 3. Clear lower bulbar conjunctiva (a) in
the right eye one month after the resection but pigmented lesions along the corneal limbus (b) relapsing
in half a year. The excision of relapsed lesion showing conjunctival malignant melanoma in situ
(c in low magnification, d in high magnification). Relatively clear lower bulbar conjunctiva just after
the excision (e) and one month later (f), 1 year from the initial visit. The pigmented lesions gradually
increase half a year after the excision (g) and 1 year later (h), 2 years from the initial visit. Scale
bar = 200 µm in c, 50 µm in d.
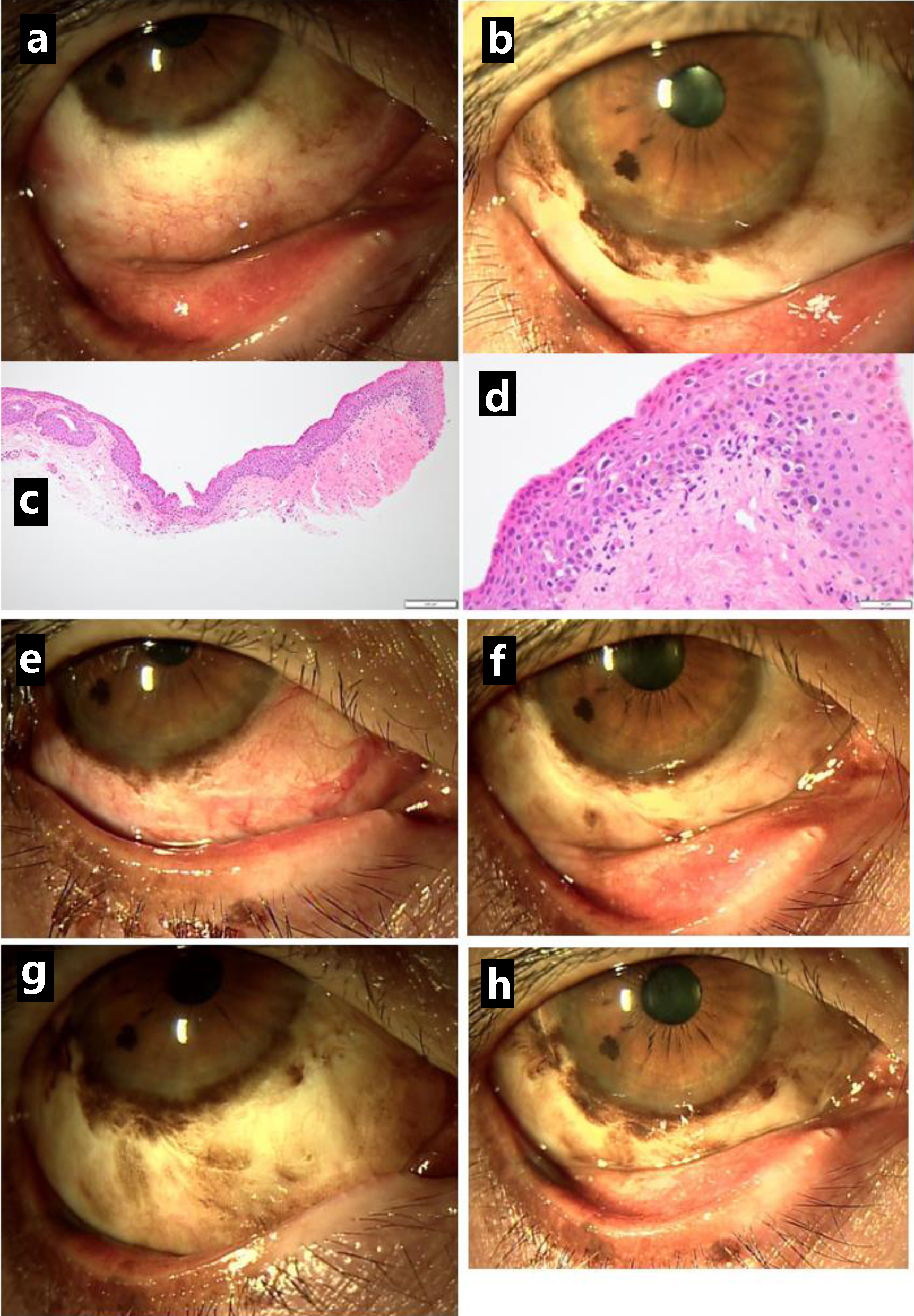
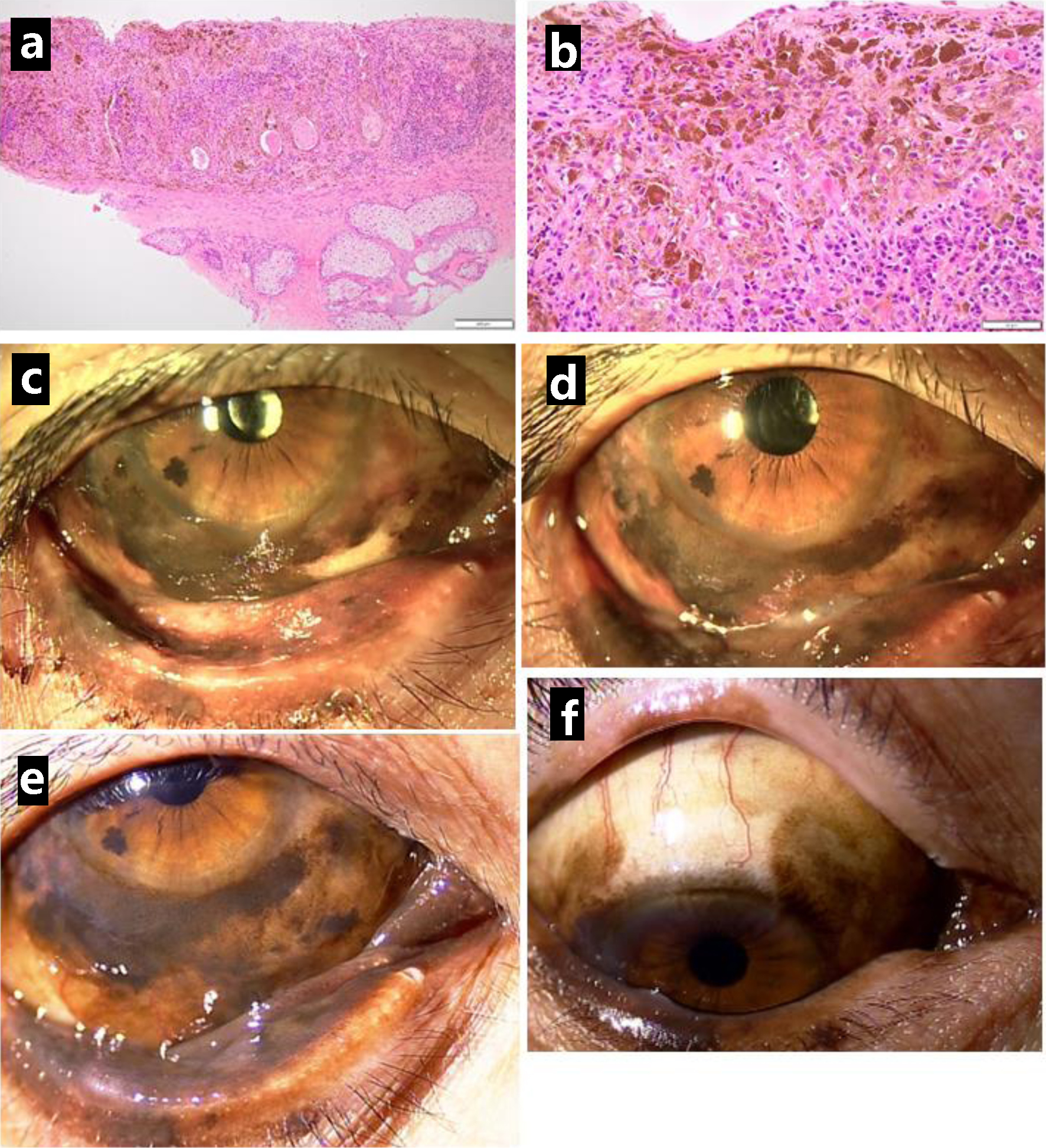
↓ Figure 4. Resection of lower eyelid-edge
pigmented lesion in the right eye, 2.5 years after the initial visit, showing malignant melanoma in
situ (a in low magnification, b in high magnification). Photos just before the resection (c) and
1 year later (d), 3.5 years from the initial visit. Pigmented lesions spreading to the lower palpebral
conjunctiva (e) and upper bulbar conjunctiva (f) half a year later, 4 years from the initial visit.
Scale bar = 200 µm in a, 50 µm in b.
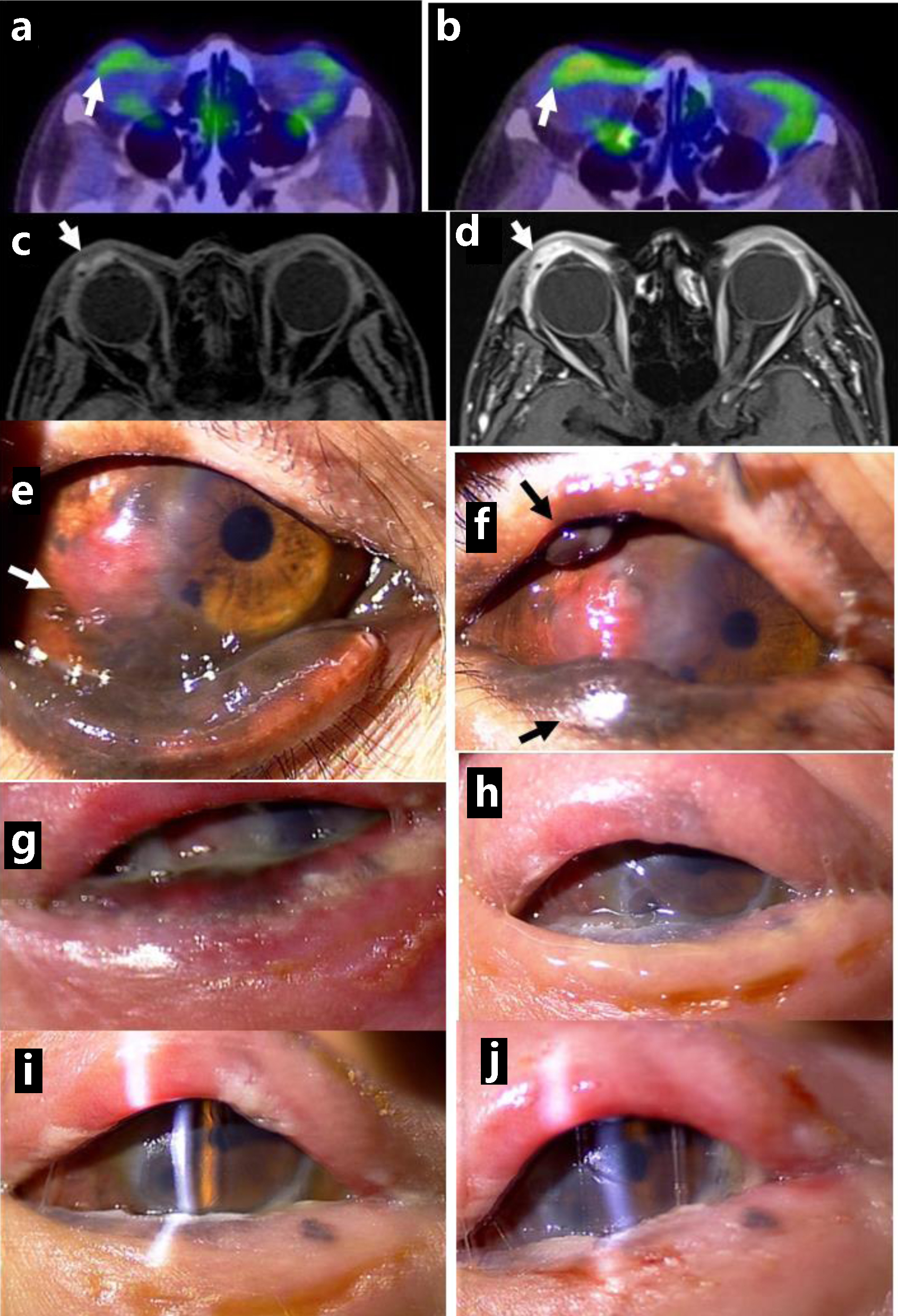
↓ Figure 5. Positron emission tomography, showing
no abnormal uptake in ocular surface of the right eye at the initial visit (arrow, a) and mildly
increased uptake 5 years from the initial visit (arrow, b). Magnetic resonance imaging with enhancement,
showing saucer-like ocular surface lesion on the right side (arrow, c) with marked enhancement in
arterial phase (arrow, d), 5.5 years from the initial visit. Non-pigmented nodular lesion on the
temporal bulbar conjunctiva along the corneal limbus (arrow, e), 5 years from the initial visit, and
pigmented nodular lesions in the upper and lower eyelids (arrows, f). 3 months later. No pigmented
lesion in the eyelids and ocular surface immediately after the completion of proton beam therapy (g), 1
month later (h), 3 months later (i), and 5 months later (j). Note clear cornea with slit-lamp
examination (i, j).