


Perioperative Care of a Pediatric Patient With Beals Syndrome
DOI:
https://doi.org/10.14740/jmc5157Keywords:
Beals syndrome, Pseudocamptodactyly, Airway management, Aortic root dilatationAbstract
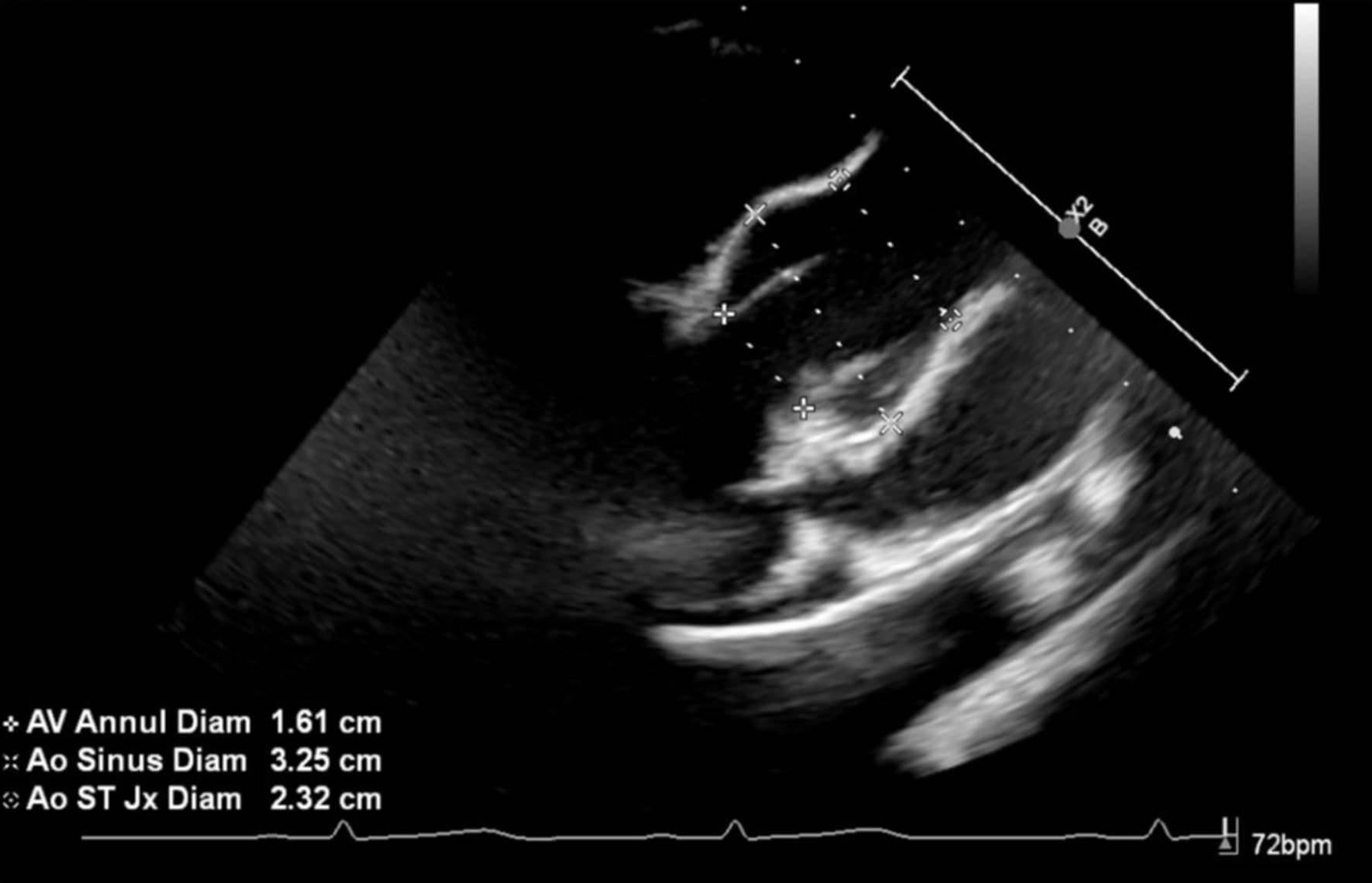
The trismus pseudocamptodactyly syndrome (Beals syndrome) is an uncommon autosomal dominant condition first described in 1971. The disorder shares phenotypic similarities with Marfan syndrome. Affected patients classically present with two main physical features: limited excursion of the mandible and flexion deformity of the fingers that occurs with wrist extension (pseudocamptodactyly). The primary cellular defect is a mutation of the fibrillin-2 (FBN2) gene on chromosome 5q23. Mutations to this gene change the structure of the FBN2 protein, decreasing the elasticity and altering the strength of microfibrils in the connective tissue. The connective tissue defect leads to short muscle tendon units, which prevent normal growth and development. We present an 11-year-old boy with Beals syndrome who presented for anesthetic care during posterior spinal fusion (PSF). To date, there are a limited number of reports in the literature outlining anesthetic care in these patients. End-organ involvement of Beals syndrome is outlined, the potential impact on perioperative care discussed, and previous reports of anesthetic care reviewed.
Published
Issue
Section
License
Copyright (c) 2025 The authors

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.






