


“False” False Tendon: Fatal Intramyocardial Dissecting Hematoma
DOI:
https://doi.org/10.14740/jmc5096Keywords:
Intramyocardial dissecting hematoma, Myocardial infarction, Cardiac imagingAbstract
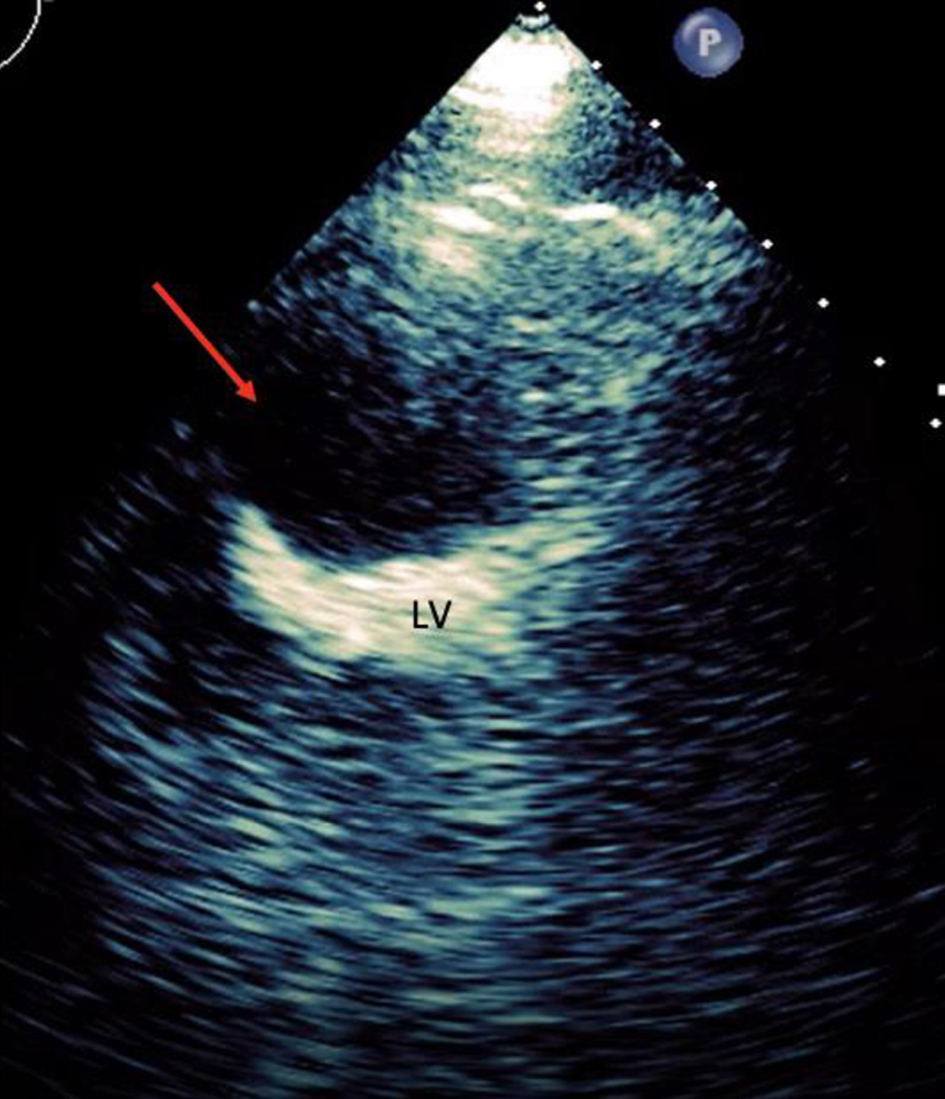
Intramyocardial dissecting hematoma (IDH) is a rare complication that may emerge from myocardial infarction, thoracic injury, or percutaneous intervention. In the past, IDH was diagnosed through surgical intervention or postmortem autopsy. We present a case of a 70-year-old male with comorbidities who admitted to the intensive care unit after suffering out of hospital pulseless electrical activity cardiac arrest and obtained return of spontaneous circulation after chest compressions. Initial electrocardiogram (ECG) showed ST elevation in the anterolateral leads. Repeated ECG a few minutes later showed junctional rhythm bradycardia with a rate of 27 and serial changes of an anterolateral infarct were present and placed on percutaneous pacing with vasopressors. The troponin I peaked at 1.880. Transthoracic echocardiography (TTE) portrayed a hyperechoic mobile filamentous structure near the cardiac apex, which was thought to be a false left ventricular (LV) tendon initially. A repeat TTE with the use of an ultrasound enhancing agent (sulfur hexafluoride) revealed an apical neocavity with no contrast filling, suggestive of a large apical IDH within the LV. The patient expired because of cardiac arrest secondary to cardiogenic shock refractory to pressor support, with no autopsy performed. This case highlights an uncommon and timelier diagnostic modality of IDH in deference of more costly and prolonged imaging studies.
Published
Issue
Section
License
Copyright (c) 2024 The authors

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.






