


A Peculiar Case of Fetal Distress Leading to the Diagnosis of Diabetic Ketoacidosis in Pregnancy
DOI:
https://doi.org/10.14740/jmc5088Keywords:
Diabetes ketoacidosis, Fetal distress, Pregnancy, Non-reassuring fetal statusAbstract
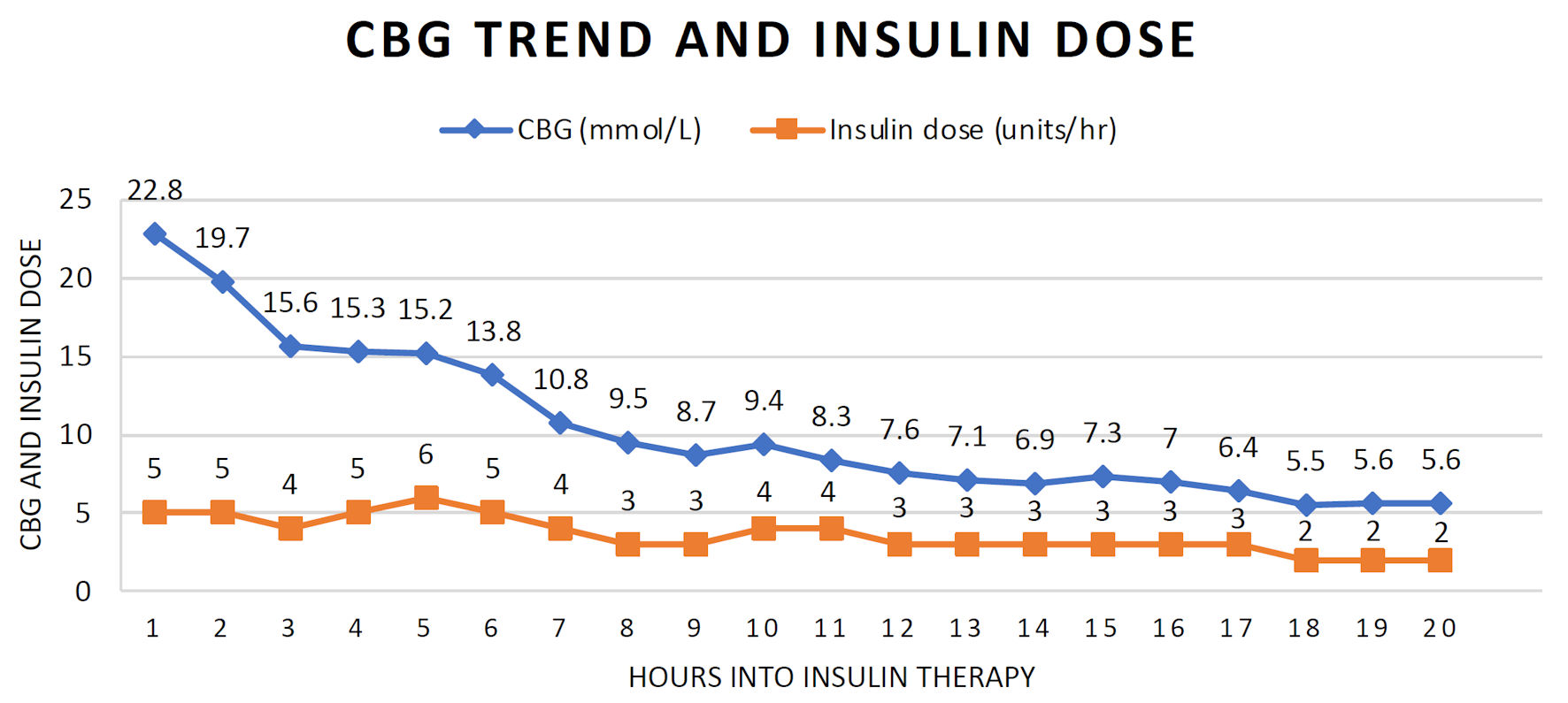
Diabetes ketoacidosis (DKA) in pregnancy is associated with significant maternal and neonatal morbidity. It is rare for women without a prior history of diabetes mellitus (DM) to develop DKA. This case report describes an atypical presentation of DKA in a 38-year-old primigravida, with no history of DM, presenting with “unexplained” fetal distress. She presented at 25 weeks to our labor ward triage with an unrelated complaint of prolapsed piles. There were no complaints of reduced fetal movement, abdominal or contraction pains or per vaginal bleeding. Ultrasonography showed an appropriately grown fetus with normal liquor volume. Incidental fetal distress was picked up on a cardiotocography (CTG) which showed a fetal heart rate of 150 beats per minute with reduced variability and shallow decelerations. The unlikely diagnosis of DKA was suspected when a random capillary blood glucose (CBG) level returned as “HI”. Investigations revealed the triad of elevated venous glucose, raised serum ketones and high anion gap metabolic acidosis (with a maternal pH of 7.14), consistent with the diagnosis of DKA. She was aggressively treated with intravenous insulin and hydration therapy. Fetal distress resolved with resolution of the DKA. She eventually delivered a healthy baby at 37-week gestation. This case raises awareness of a rare occurrence of DKA in late pregnancy as the first presentation of DM and highlights the importance of considering a hyperglycemic crisis as a potential cause of a suspicious CTG in an asymptomatic woman without any clear reason for fetal distress. Timely diagnosis and prompt treatment of the underlying condition is lifesaving, and avoids urgent delivery and risks associated with prematurity.
Published
Issue
Section
License
Copyright (c) 2025 The authors

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.






