| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://jmc.elmerpub.com |
Case Report
Volume 16, Number 6, June 2025, pages 226-231

B-Cell Lymphoma Presenting as a Pancreatic Mass
Sondos Badrana, Alexander T. Phana, Adelle Kananb, Viet-Tien Nguyenb, Katherine Bourbeau-Medinillaa
aDepartment of Internal Medicine, Arrowhead Regional Medical Center, Colton, CA 92324,
USA
bSchool of Medicine, California University of Science and Medicine, Colton,
CA 92324, USA
cCorresponding Author: Sondos Badran, Department of Internal
Medicine, Arrowhead Regional Medical Center, Colton, CA 92324, USA
Manuscript submitted November 18, 2025, accepted March 29, 2025, published online June 30,
2025
Short title: B-Cell Lymphoma as a Pancreatic Mass
doi:
https://doi.org/10.14740/jmc5086
| Abstract | ▴Top |
Non-Hodgkin lymphoma (NHL) has many subtypes, with diffuse large B-cell lymphoma being the most common subtype. Typical symptoms of NHL include fever, weight loss, night sweats, and lymphadenopathy. Treatment depends on the subtype of NHL. Our case presents the clinical course of a patient who presented with obstructive jaundice and pancreatitis rather than typical symptoms of NHL. Workup included abdominal imaging showing a pancreatic mass and biopsy ultimately revealed high-grade B-cell lymphoma. This case presents a rare diagnosis of likely primary pancreatic lymphoma.
Keywords: B-cell lymphoma; Non-Hodgkin lymphoma; Jaundice; Primary pancreatic lymphoma
| Introduction | ▴Top |
Non-Hodgkin lymphoma (NHL) is the most common hematological malignancy in the world, comprising about 2.8% of worldwide cancer diagnoses [1]. Typically, NHL occurs in lymphoid tissue, but a considerable portion of the disease arises from non-lymphoid tissue. These primary extranodal lymphomas are estimated to make up at least one-fourth of lymphomas [2]. The gastrointestinal tract is the most common extranodal site for NHL, with the stomach and small intestine at the forefront of cases [3]. Less typically involved is the pancreas; it may be secondarily involved in patients with NHL, but primary occurrence is exceedingly rare. Primary pancreatic lymphoma (PPL) makes up fewer than 2% of extranodal NHLs and less than 0.5% of all pancreatic tumors overall [4].
Diagnosing PPL poses challenges, as presenting symptoms are variable and often nonspecific. Most patients with PPL initially present with abdominal pain or an abdominal mass, but other symptoms include weight loss, jaundice, pancreatitis, and diarrhea [3]. Clinicians may initially be concerned about pancreatic adenocarcinoma in these patients, especially due to the significant overlap of vague presenting symptoms between the two pathologies [5]. Apart from the rarity and generalized symptomatology of PPL, there is an additional layer of difficulty when it comes to recognizing the disease. It typically lacks the classic B symptoms of nodal NHL, such as fever, chills, and night sweats, making it even more elusive [3]. Here, we report the case of a 64-year-old patient who presented primarily with obstructive jaundice secondary to a pancreatic mass and was subsequently diagnosed with B-cell lymphoma of the pancreas following tissue biopsy.
| Case Report | ▴Top |
Investigations
The patient is a 64-year-old female with no prior medical history who presented due to 1 week of epigastric pain associated with non-bilious, non-bloody vomiting. Her symptoms of pain and vomiting were worse at night. The pain was described as non-radiating and rated a 10 out of 10 intensity. She had not seen a primary care physician since she was a child and had poor medical follow-up. She otherwise denied fevers, night sweats, weight loss, changes in bowel habits, chest pain, and dyspnea. She denied family history of malignancy. She did not take any medications prior to her hospital presentation.
Diagnosis
In the emergency department (ED), vital signs included a blood pressure of 126/76 mm Hg, heart rate of 73 beats per minute, temperature of 97.5 °F, respiratory rate of 16, and oxygen saturation of 96% on room air. A physical exam was notable for generalized jaundice, mild scleral icterus, dry mucous membranes, and epigastric tenderness to light and deep palpation. In the ED, a computed tomography (CT) of the abdomen and pelvis with intravenous (IV) contrast demonstrated an 8 cm pancreatic mass involving the head and uncinate process causing biliary obstruction of the common bile duct (CBD) with mesenteric lymphadenopathy; the mass also encased the superior mesenteric vein, splenic vein, and proximal portal vein (Figs. 1 and 2).
 Click for large image |
Figure 1. Axial section of a computed tomography of the abdomen demonstrating an 8 cm pancreatic mass, indicated by the arrow. |
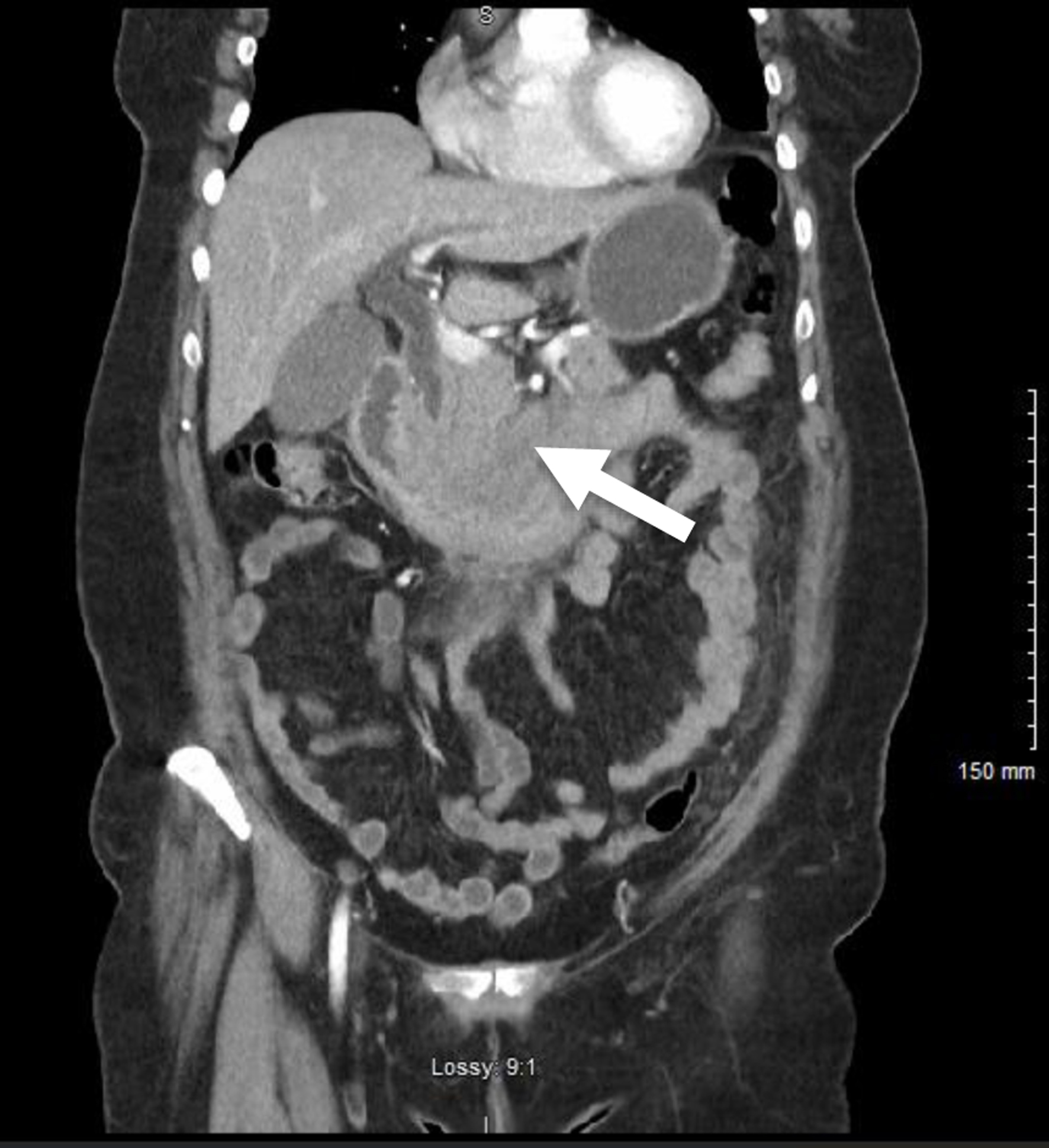 Click for large image |
Figure 2. Coronal section of a computed tomography demonstrating a pancreatic mass, indicated by the arrow. |
Initial laboratory studies were notable for hypokalemia, hypochloremia, elevated lipase, elevated alkaline phosphatase, elevated aspartate aminotransferase (AST), elevated alanine aminotransferase (ALT), and direct hyperbilirubinemia (Table 1). A lipid profile did not demonstrate significant hypertriglyceridemia. Carcinoembryonic antigen was normal (1 ng/mL, N: 0 - 3 ng/mL), alpha-fetoprotein was undetectable (N < 8 ng/mL), but carbohydrate antigen 19-9 (CA19-9) was elevated at 155 (N < 34 U/mL). Hepatitis A IgM, hepatitis B surface antigen, hepatitis B core IgM, and hepatitis C total antibody were all non-reactive. At this time, the suspicion for pancreatic adenocarcinoma was high due to its presentation and elevated CA19-9.
 Click to view |
Table 1. Initial Laboratory Studies Performed
in the Emergency Department |
Treatment
The patient was given IV fluids and opioids for pain control in the setting of pancreatitis. Gastroenterology and Surgical Oncology were consulted. A magnetic resonance cholangiopancreatography (MRCP) demonstrated a pancreatic head mass encasing vascular structures with marked CBD dilation up to 15 mm. An endoscopic ultrasound (EUS) was performed, demonstrating CBD obstruction, dilated intrahepatic ducts, pancreatic duct dilation, a hypoechoic heterogenous mass measuring 54 × 43 mm in the head of the pancreas with encasement of the portal vein. During the EUS, the mass was biopsied successfully and rapid on-site evaluation deemed the sample adequate for diagnosis. Additionally, esophagitis and duodenal stenosis were noted, so the endoscopic retrograde cholangiopancreatography (ERCP) was unable to be successfully performed. Subsequently, the patient underwent a percutaneous transhepatic cholangiography with successful placement of a biliary drain for decompression.
Pathological studies demonstrated a high-grade B-cell lymphoma (positive CD45, CD20, CD10, BCL-2, and BCL-6; negative for pancytokeratin, CD5, CD43, BCL-1, C-Myc, MUM1, EBER ISH). A bone marrow biopsy of the iliac crest was negative for malignant lymphoma, cytopenias, anemia, immature blasts, or increase in plasma cells. On hospital day 15, the patient’s abdominal pain resolved and all prior laboratory abnormalities had reduced (bilirubin and liver function tests), demonstrating resolution of her original presenting obstructive pattern. She was discharged with a biliary drain in place, with plans to follow-up with outpatient primary care, medical oncology, and surgical oncology.
Follow-up and outcome
In the outpatient setting, oncology started the patient on a three-cycle regimen of polatuzumab, rituximab, cyclophosphamide, doxorubicin, and prednisone. However, she developed neutropenic fever twice, so she was transitioned to a reduced dose combination of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP), without further admissions for neutropenic fever. At 6 months follow-up, the patient is alive and well. Her biliary drain stopped draining fluid, and she is undergoing evaluation for drain removal.
| Discussion | ▴Top |
Pancreatic malignancies are the fourteenth most common cancer worldwide, with pancreatic adenocarcinoma being the most common pancreatic malignancy. PPL is an extremely rare form of pancreatic cancer, accounting for 0.2% of all pancreatic tumors, 0.6% of extranodal lymphomas, and 0.1% of malignant lymphomas [6, 7]. PPL typically affects males in the fifth or sixth decade of life [8]. Presentation of PPL is non-specific. The most common reported symptom is abdominal pain (83%), followed by weight loss (50%) and jaundice (37%). Unique symptoms that patients with PPL present are acute pancreatitis (12%), small bowel obstruction (12%), and diarrhea (12%) [6, 9]. B-symptoms, including fever, night sweats, and weight loss, are uncommon findings in PPL, occurring in less than 2% of reported cases.
Laboratory results are also non-specific in PPL. Elevated bilirubin, AST, and ALT are common laboratory findings, which demonstrates obstructive pattern [7]. Facchinelli et al analyzed 162 patients with PPL, 43% of patients had elevated lactate dehydrogenase (LDH) and 28% had elevated CA19-9 tumor marker [9]. LDL increase is common in PPL and associated with a worse prognosis [4, 8]. CA19-9 is not commonly elevated when compared to pancreatic adenocarcinoma. CA19-9 can be increased if there is biliary obstruction in PPL.
Our patient described in this case report presented with non-specific symptoms. Her main complaints included abdominal pain, vomiting, and jaundice. The patient’s symptoms were also consistent with pancreatitis, which is a less common. Furthermore, laboratory work demonstrated an obstructive pattern with elevated bilirubin, AST, and ALT. LDH and CA19-9 were also elevated. These findings are similar and consistent with previously described cases. The patient’s age also fits the typical description, which occurs in the fifth or sixth decade of life. However, the patient’s gender is not typically associated with PPL, as our patient is female, and PPL is a generally male predominant condition.
Imaging is vital in the diagnostic process. Unfortunately, distinguishing between PPL and pancreatic adenocarcinoma is challenging. On imaging, PPL usually has a large tumor usually greater than 5 cm when compared to pancreatic adenocarcinoma [8]. Similar to adenocarcinoma, PPL is localized to the head of pancreas in 63% of cases [4, 6]. To determine diagnosis, CT or EUS with biopsy should be performed. CT and EUS-guided biopsy have similar sensitivity. However, EUS has higher specificity and usually the preferred method for sampling pancreatic tissue [8].
The patient discussed had imaging findings consistent with previous literature. The patient had a bulky tumor on CT, which was 8 cm involving the pancreatic head and an uncinate process. Although there were concerns for pancreatic adenocarcinoma given elevated CA19-9, which is more common in pancreatic adenocarcinoma, EUS with biopsy was then performed. EUS pathology findings were consistent with B-cell lymphoma.
After diagnosis, chemotherapy should be initiated without delay, as occurred with our patient. This differs from primary adenocarcinoma, where surgery is the best modality of treatment [10]. Common chemotherapy drugs include R-CHOP [8, 11].
PPL should always be on the differential when identifying pancreatic lesions. The patient in this case report presenting with painless jaundice and elevated CA19-9 pointed towards a more likely diagnosis of pancreatic adenocarcinoma. With further imaging and biopsy, PPL was diagnosed. In addition to imaging, demographics should be considered as PPL occurs mostly in males; however, our patient is female, which differed from previous literature. Thorough diagnostic investigation of pancreatic lesions further to determine if it is truly PPL versus primary adenocarcinoma is crucial as the prognosis differs significantly. Patients with pancreatic adenocarcinoma have a 5-year survival of 5%, in comparison to PPL, which has a 30% cure rate [10]. Although our patient discussed in this case report had similar findings to previous case reports, this paper highlights the importance of having a broad differential in patients presenting with similar symptoms to that of primary adenocarcinoma.
Learning points
This case highlights a rare presentation of a PPL with elevated CA19-9 levels. Though this is not unheard of, its rare presentation should be noted, as clinicians commonly suspect pancreatic adenocarcinoma rather than PPL. As such, clinicians should include this in the differential diagnosis when a patient presents with obstructive jaundice that is concerning for pancreatic malignancy. Future research may investigate definitive risk factors that may predict extranodal NHLs and the most optimal treatment regimen for pancreatic lymphoma.
Acknowledgments
The authors would like to thank and express their gratitude to Arrowhead Regional Medical Center’s exceptional medical staff for their clinical support.
Financial Disclosure
No funding was involved in this case study.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. The patient was also appropriately de-identified for this manuscript.
Author Contributions
Dr. Sondos Badran, Dr. Alexander Phan, Adelle Kanan, and Viet-Tien Nguyen contributed to the initial manuscript write-up, literature review, and editing of the manuscript. Dr. Katherine Bourbeau-Medinilla attended on the case and contributed to editing of the manuscript.
Data Availability
All data in our report were obtained from the patient’s hospitalization. Any inquiries regarding supporting data availability of this study should be directed to the corresponding author.
Abbreviations
ALT: alanine aminotransferase; AST: aspartate aminotransferase; CBD: common bile duct; CT: computed tomography; ED: emergency department; ERCP: endoscopic retrograde cholangiopancreatography; EUS: endoscopic ultrasound; IV: intravenous; LDH: lactate dehydrogenase; MRCP: magnetic resonance cholangiopancreatography; NHL: non-Hodgkin lymphoma; PPL: primary pancreatic lymphoma; R-CHOP: rituximabcyclophosphamide, doxorubicin, vincristine, and prednisone
| References | ▴Top |
- Thandra KC, Barsouk A, Saginala K, Padala SA, Barsouk A, Rawla P.
Epidemiology of non-Hodgkin's lymphoma. Med Sci (Basel). 2021;9(1):5.
doi pubmed - Zucca E, Roggero E, Bertoni F, Cavalli F. Primary extranodal
non-Hodgkin's lymphomas. Part 1: Gastrointestinal, cutaneous and genitourinary lymphomas. Ann
Oncol. 1997;8(8):727-737.
doi pubmed - Saif MW. Primary pancreatic lymphomas. JOP.
2006;7(3):262-273.
pubmed - Ullah A, Lee KT, Malham K, Yasinzai AQK, Tareen B, Lopes D, Wali A,
et al. Pancreatic diffuse large B-cell lymphoma in the US population. Cureus.
2023;15(6):e39862.
doi pubmed - Risch HA, Yu H, Lu L, Kidd MS. Detectable symptomatology preceding
the diagnosis of pancreatic cancer and absolute risk of pancreatic cancer diagnosis.
Am J Epidemiol. 2015;182(1):26-34.
doi pubmed - Shnitser A, Halegoua-DeMarzio D, Loren DE. Primary pancreatic
lymphoma presenting as acute pancreatitis. Gastroenterol Hepatol (N Y).
2016;12(7):456-458.
pubmed - Lamrani FZ, Amri F, Koulali H, Mqaddem OE, Zazour A, Bennani A,
Ismaili Z, et al. Primary pancreatic lymphoma: Report of 4 cases with literature review. Radiol
Case Rep. 2024;19(1):70-77.
doi pubmed - Rad N, Khafaf A, Mohammad Alizadeh AH. Primary pancreatic lymphoma:
what we need to know. J Gastrointest Oncol. 2017;8(4):749-757.
doi pubmed - Facchinelli D, Sina S, Boninsegna E, Borin A, Tisi MC, Piazza F,
Scapinello G, et al. Primary pancreatic lymphoma: Clinical presentation, diagnosis, treatment,
and outcome. Eur J Haematol. 2020;105(4):468-475.
doi pubmed - Tikue A, Bedanie G, Brandi L, Islam S, Nugent K. Primary pancreatic
large B-cell lymphoma presenting as acute pancreatitis. Cureus. 2020;12(8):e9583.
doi pubmed - Ponugoti S, Dhakal B, Pawa S. A rare case of diffuse large B cell lymphoma of pancreas presenting as acute pancreatitis: 248. American Journal of Gastroenterology. 2013;108:S76-S77.
This
article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0
International License, which permits unrestricted non-commercial use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Journal
of Medical Cases is published by Elmer Press Inc.